- Traumatic Vascular Injury Toolkit
A high degree of suspicion for vascular injury (traumatic aneurysms, arteriovenous fistula, venous injury) should accompany all patients who present with pTBI. Most specifically, those with penetration through areas of high vascular concentration (trans-orbital, pterional, bi-hemispheric, posterior fossa), violation of multiple dural compartments, and intracerebral hematoma are considered highest risk for vascular injury (Section VI-7, Neurovascular Imaging). With this in mind, investigation to rule out CV injury should be performed in all patients with penetrating brain injury (Section VI-7, Neurovascular Imaging; Section VII-6 Open and Endovascular Management of Traumatic Vascular Injury)
10-20,24,38,64,77,79,112-124 . CTA is an adequate modality to rapidly rule out larger traumatic aneurysms at initial presentation, and should be performed as an initial diagnostic screening tool for all patients with pTBI11,13,77 . It must be remembered that the diagnostic sensitivity of CTA is hampered by beam hardening artifact from retained penetrating metallic fragments, and therefore a follow up diagnostic cerebral angiogram is recommended for most patients with severe pTBI Section VI-7, Neurovascular Imaging, Level II)13 .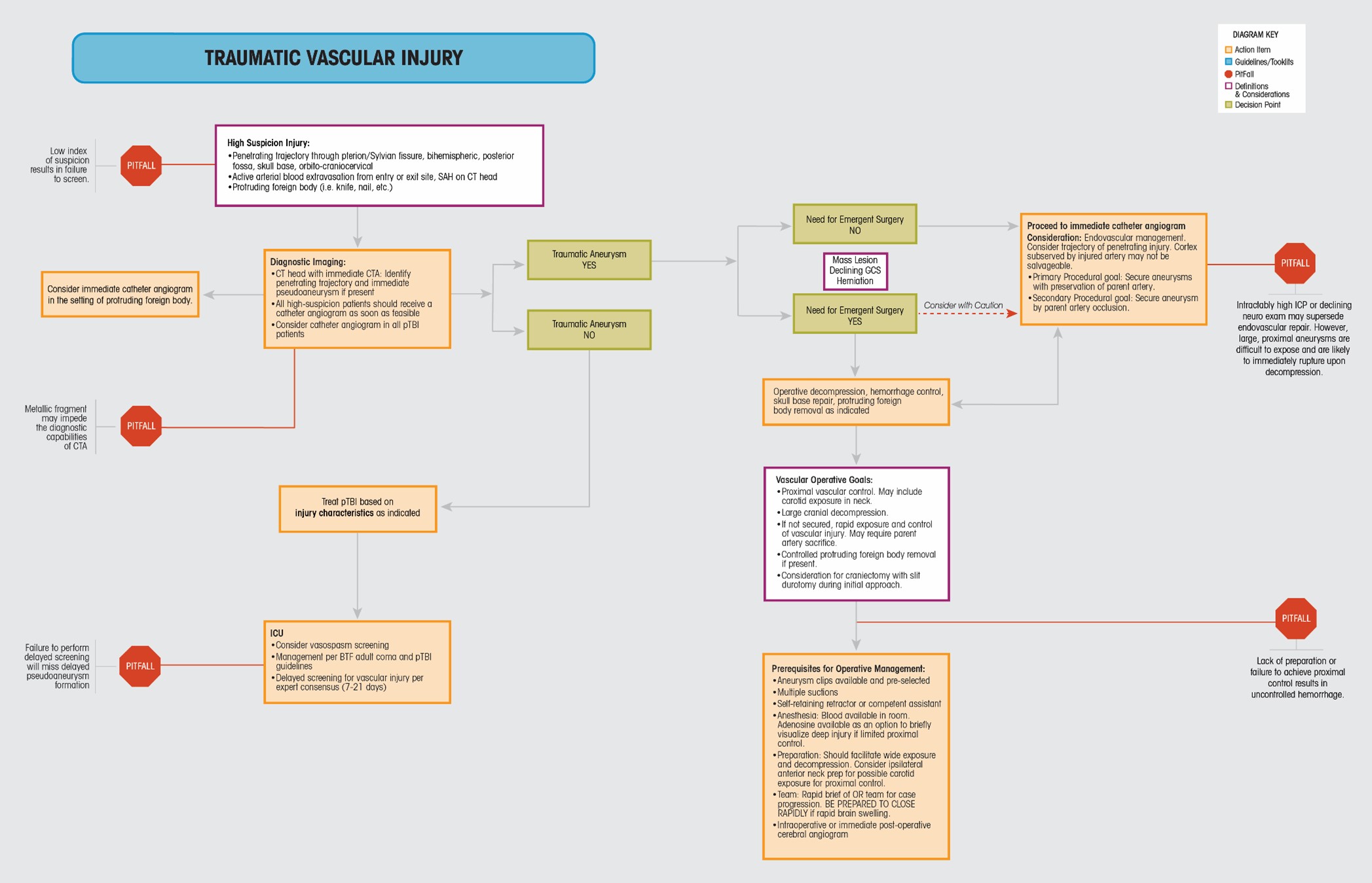
Following initial screening, it is the presence or absence of traumatic vascular injury, specifically traumatic aneurysms, their size, and their location that should influence further surgical decision making. In general, small, distal (M4, A4) traumatic aneurysms may be addressed during surgical exposure for decompression, and will almost always include sacrifice of the associated artery. Smaller, proximal traumatic aneurysms may not rupture upon opening, and may be possible to address endovascularly in a delayed fashion.
The most concerning circumstance involves the formation of a large, skull base traumatic aneurysm (ICA, M1 MCA, A1 ACA, vertebrobasilar) associated with severe cerebral injury requiring urgent decompression. What is the most appropriate course of action? Should the aneurysm be addressed first followed by decompression, or vice versa. Concerning the traumatic aneurysm, it must be remembered that these are not true saccular aneurysms. They are most often circulating blood encapsulated by coagulum. Open surgical approaches to these injuries are significantly hampered by anatomic disruption from the penetrating injury trajectory, cerebral swelling and edema, and hematoma. If immediate surgical decompression is considered necessary in the non-medically futile patient, the surgeon should expect and prepare for immediate and brisk arterial bleeding with opening. Adequate and running supply of blood products should be present in the room. Aneurysm clips, emergency suction, and a competent assistant should be present. A cerebrovascular subspecialized neurosurgeon may be very valuable in such a case if available. Neck preparation and exposure for proximal control may be necessary. The surgeon should also prepare to sacrifice the injured artery given reconstruction options are unlikely to be successful in this setting. Surgical bypass may be possible in this setting if performed by a highly experienced surgeon with assistance. Alternatively, strong consideration for endovascular management in this situation should be entertained. It may be possible to provide some protection by endovascular means, but at the cost of delaying cranial decompression. Overall, the decision in this "worst case scenario" remains the responsibility of the operative surgeon, and should be accompanied by rapid, thoughtful preparation with either chosen course of action.
In general, it is possible to treat traumatic aneurysms using endovascular techniques. Coil occlusion of traumatic aneurysms is possible, and should be entertained if considered appropriate
16,17,116-118,122,123 . For those aneurysms that present on large, skull base conducting vessels, or for those traumatic aneurysms that have recurred after initial treatment, flow diversion may be an option113 . Because this approach requires some form of dual anti-platelet therapy for an extended period of time (3-6 months), timing of this approach must take into account the need for additional open surgical procedures.Should vascular injury be diagnosed and treated, a follow up cerebral angiogram 7-21 days after the aneurysm is diagnosed and treated, is recommended.
- Traumatic Vascular Injury ToolkitTraumatic Vascular Injury
High Suspicion Injury:
- Penetrating trajectory through pterion/Sylvian fissure, bihemispheric, posterior fossa, skull base, orbito-craniocervical
- Active arterial blood extravasation from entry or exit site, SAH on CT head
- Protruding foreign body (i.e. knife, nail, etc.)