Once a Futility Assessment has been completed, a determination must be made concerning the type and timing of surgical intervention. This decision relies heavily upon the extent of injury. As previously stated, unless judged medically futile, pTBI is almost always a surgical disease. Interventions could range from local debridement and closure to complex skull base reconstructions with need to address penetrating cerebrovascular injury.
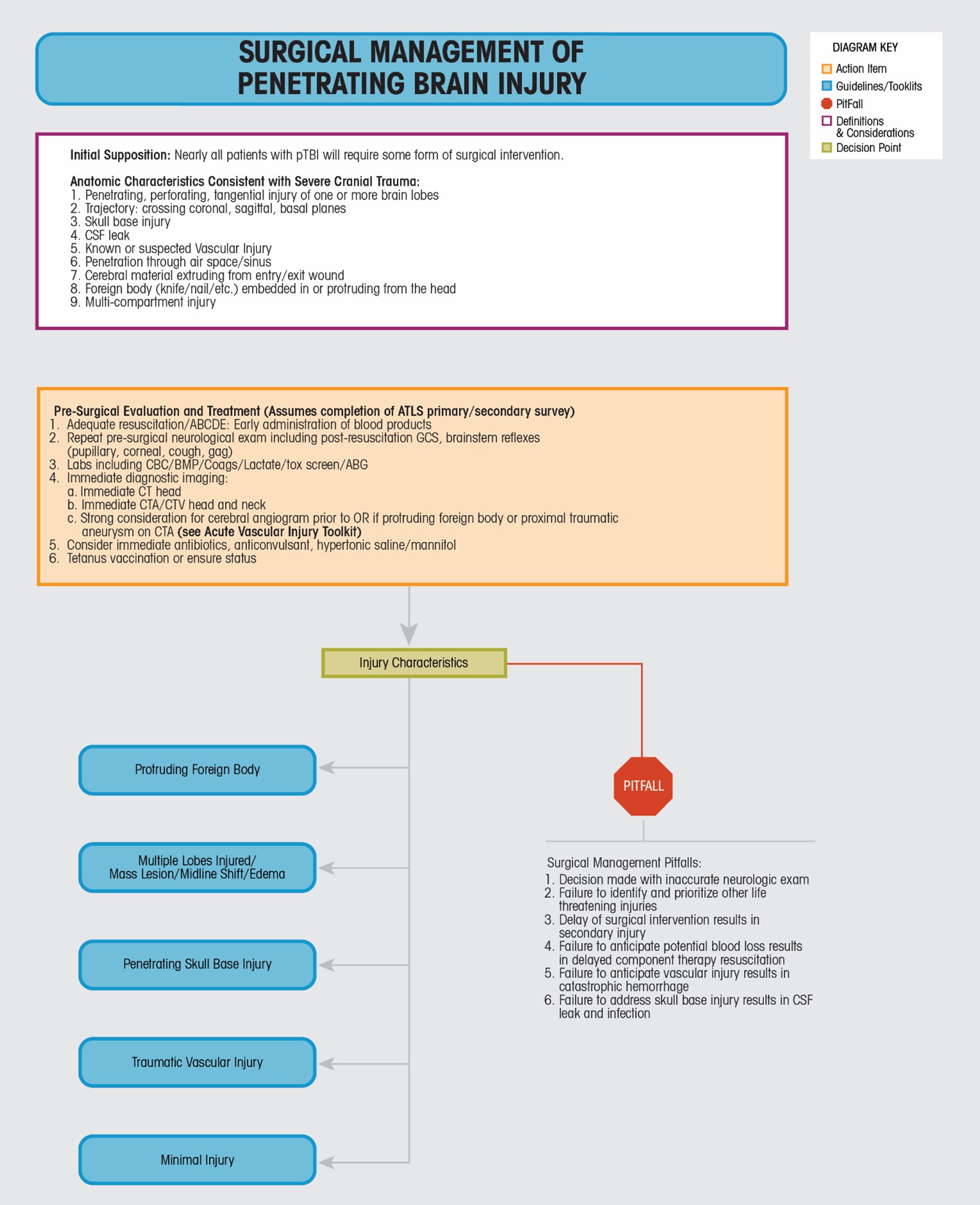
The Surgical Management Toolkit provides a broad overview of the anatomic characteristics associated with severe cranial trauma, pre-surgical evaluation and treatment, the general injury categories associated with pTBI, and, unique to this algorithm, pitfalls that a clinician should make every effort to avoid. Determination of the type and extent of injury relies heavily upon the patient's physical examination (GCS, external injury patterns) and imaging that should initially include CT and CTA of the head/neck. Five general injury categories are provided with representative imaging for reference. It is important to note that a patient may fall into one category, or nearly all categories. For example, a patient who presents with a knife protruding from the orbit has an obvious protruding foreign body, may have an expanding intracranial mass lesion in the form of a hematoma, anterior skull base disruption, and traumatic vascular injury to the internal carotid artery. It is the responsibility of the treating neurosurgeon to anticipate these injuries based on their personal physical examination and review of imaging, and act accordingly.
Should surgical intervention be considered necessary, there are two points that should be stressed. First, surgical repair of severe penetrating brain injury is often associated with significant blood loss. The neurosurgeon should strongly consider resuscitation with component therapy (PRBC:FFP:Plt in 1:1:1 ratio or whole blood transfusion) prior to operative intervention in anticipation of this loss. Preparations for severe blood loss should be made such as alerting to the possible need to initiate a massive transfusion protocol, availability of a rapid transfuser and aneurysm clips as well as need to establish proximal vascular control (perhaps by prepping the neck or having an endovascular balloon ready to occlude the carotid) or to have the assistance of an expert cerebrovascular neurosurgeon. This often starts in the trauma bay or in transport to the operating room. Second, should surgery be deemed necessary, it should proceed as soon as possible or considered safe (Section VII-1, Urgency of Neurosurgery, Consensus and Evidence Based Recommendations)44,53-57. For example, a patient with a GCS of 6T with brain, blood, and CSF egressing from a cranial exit wound will likely require immediate cranial decompression regardless of the time of presentation. A patient with penetrating skull base injury with orbital and sinus involvement, with a possible skull base traumatic aneurysm on CTA may require cerebral angiography and endovascular intervention along with subsequent multi-disciplinary skull base and orbital reconstruction (See Traumatic Vascular Injury Toolkit). This may take time to assemble from a team perspective.
The following sections provide specific guidance tailored to the type of injury.