Inadequate component resuscitation results in intraoperative hypotension from blood loss.
- Severe Injury (Multiple Lobes Injured/Mass Lesion/Midline shift/Edema) Toolkit
High velocity pTBI is often associated with significant cerebral injury. Initial presentation may be characterized best by the wounding trajectory. If the patient survives, significant cerebral edema and swelling can be anticipated over the early days following the initial injury secondary to the primary and secondary ballistics cavities
74,75 . For the purposes of this algorithm, the term "multiple lobes" is defined as a penetrating injury with trajectory that traverses more than one lobe or cerebral compartment. Cerebral injury of this type can be associated with a mass lesion, usually defined as a hematoma, midline shift, and cerebral edema. As with all trauma evaluations, the initial physical examination is crucial. Localization of the entry, and if applicable, exit wound(s) is critical as this will inform understanding of possible missile/fragment primary trajectories. Rapid CT and CTA should be obtained as soon as safe and feasible in order to determine additional extent of injury, including any secondary trajectories, skull base injury, and CTA detectable vascular injury (traumatic aneurysms, arterial occlusions)10,76-79 . It is worth noting that injury to the skull base and cerebral vasculature may accompany severe cerebral injury, and therefore the Skull Base Injury and Traumatic Vascular Injury Toolkits may require consultation.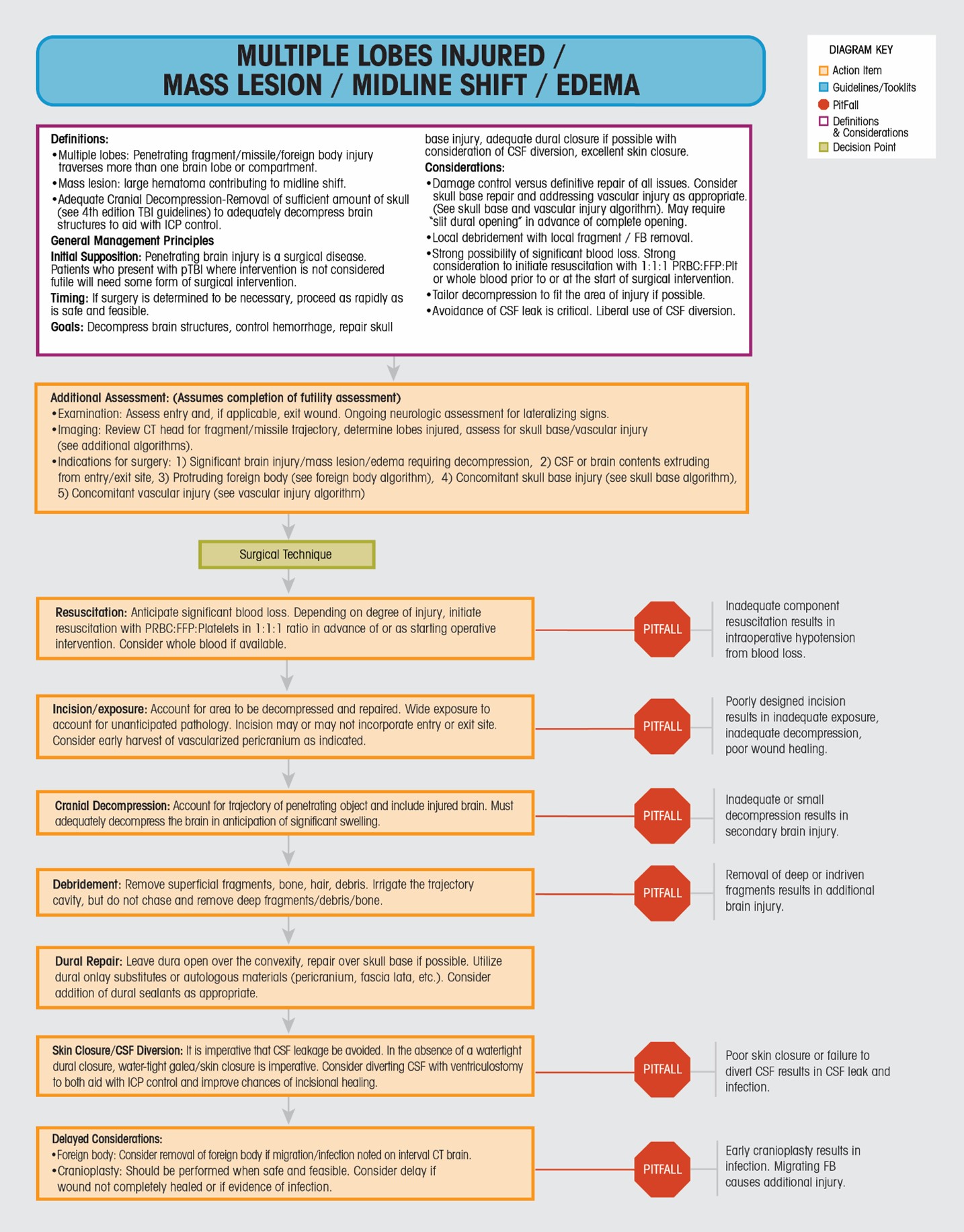
Pending a Futility Assessment, injury of this type will almost certainly require surgical intervention. If surgery is deemed necessary, there is little benefit to delay (VII-1 Urgency of Neurosurgery, Level IV and expert consensus)
44,53-57 . One report recommends surgery within 5 hours if possible to improve outcomes80 . Resuscitation consisting of PRBC:FFP:Plt in a 1:1:1 ratio or whole blood should begin en route to or immediately upon arrival to the operating room in anticipation of significant blood loss81,82 . The goals of surgery depend largely on the location and extent of injury, and include cerebral decompression, debridement of local bone/foreign bodies/hair, etc., and control of hemorrhage (Section VII-3, Extent of Debridement). The surgical plan depends heavily on the wounding pattern. For example, a unilateral supratentorial GSW to the brain with retained missile may be best addressed with a unilateral exposure. A bifrontal injury may be best addressed with a bifrontal exposure. In any case, the approach should account for a large decompression with planned craniectomy if cerebral swelling or edema is present or anticipated (Section VII-1, Urgency of Neurosurgery, Level IV). The decision to save or discard the bone may depend heavily on the degree of foreign body contamination or disruption seen at the initial surgery. Debridement of locally indriven bone, foreign bodies, and hair is appropriate, and this can be facilitated by irrigation of the missile/fragment tract. It is not necessary, and may be detrimental, to search for and remove deeply indriven fragments and bone (Section VII-3, Extent of Debridement, Level III)23,25,30,37,60,61,63,66,83-92 . Following decompression, control of hemorrhage, and local debridement, dural and skin closure is necessary. Every effort should be made to avoid cerebrospinal fluid leak from the skin in order to prevent infection (Section VII-4, Prevention and Management of Cerebrospinal Fluid Leaks, Level II, Consensus)53,59-72,93 . It is often not possible to obtain a watertight dural closure. Dural onlay with either synthetic dural replacements, pericranium or other tissue substitutes (fascia lata, etc), and/or dural sealants will likely be necessary. Subgaleal and, if possible, ventricular drain placement may facilitate and maintain the necessary multilayer, water tight skin closure.Certain circumstances require additional guidance and explanation. The presence of skull base injury, protruding foreign bodies, and cerebrovascular arterial injury will be addressed in specific Toolkits/Algorithms. Occasionally, the penetrating trajectory will include one or more dural venous sinuses. This will present with noticeable transcutaneous blood loss from the entry and/or exit wound, sinus disruption on CT/CTA, or in the operation room following exposure and decompression. There are numerous published and well-established techniques addressing the management of venous sinus injury and/or violation (Section VII-8, Management of Penetrating Venous Sinus Injuries, Level IV, Consensus)
66,67,94-98 . In general, significant blood loss should be anticipated, with blood product transfusions initiated prior to surgical repair. Standard techniques including elevating the sinus injury above the heart, but with irrigation and covering the area of injury with a wet sponge to reduce the risk of air embolism should be employed. Direct insertion of balloon catheters (foley, etc.) proximal and distal to the area of sinus laceration may help control catastrophic hemorrhage and facilitate repair94 . Injuries to the anterior third of the superior sagittal sinus may be addressed with sinus ligation if direct repair is not possible. Efforts including direct repair, tissue patch (pericranium, muscle, other tissue), dural inversion, or, less commonly, venous graft, should be made to preserve and maintain the middle to posterior third of the superior sagittal sinus if possible. Repair and preservation of the dominant transverse sinus, if known, is preferable, though ligation may also be necessary. Endovascular interventions in this setting may include delayed thrombectomy should malignant edema and cerebral infarction present in a delayed fashion97 .While it is not necessary to remove deeply indriven missile or metallic fragments at the time of initial surgical decompression (see above), delayed removal may be necessary if the fragment becomes infected or migratory
99 . Migration patterns include intraventricular, subarachnoid, within the missile/fragment tract, within a developing abscess or infection, and intravascular. Follow up imaging is necessary to ensure missile/fragment stability. A mobile fragment, depending on location and eloquence of surrounding brain, may require delayed removal.If decompressive craniectomy is performed at the first operation, delayed cranial reconstruction will be necessary. It may be necessary, given significant contamination or fragmentation, to discard the removed autologous bone. Use of synthetic cranioplasty materials may be necessary at the time of reconstruction. The literature currently does not support optimal timing for cranial reconstruction in the setting of closed and penetrating brain injury (Section VII-9, Timing of Cranioplasty, Consensus)
100-103 . Prudence and judgement should be exercised with respect to timing to reduce the risk of infection while simultaneously reducing the risk of post-craniectomy syndrome of the trephined. - Severe Injury (Multiple Lobes Injured/Mass Lesion/Midline shift/Edema) ToolkitMultiple Lobes Injured / Mass Lesion / Midline Shift / Edema
Definitions:
- Multiple lobes: Penetrating fragment/missile/foreign body injury traverses more than one brain lobe or comportment.
- Mass lesion: large hematoma contributing to midline shift.
- Adequate Cranial Decompression-Removal of sufficient amount of skull (see 4th edition TBI guidelines) to adequately decompress brain structures to aid with ICP control.
General Management Principles
Initial Supposition: Penetrating brain injury is a surgical disease. Patients who present with pTBI where intervention is not considered futile will need some form of surgical intervention.
Timing: If surgery is determined to be necessary, proceed as rapidly as is safe and feasible.
Goals: Decompress brain structures, control hemorrhage, repair skull base Injury, adequate dural closure if possible with consideration of CSF diversion, excellent skin closure.
Considerations:
- Damage control versus definitive repair of all issues. Consider skull base repair and addressing vascular Injury as appropriate. (See skull base and vascular injury algorithm). May require 'slit dural opening' in advance of complete opening.
- Local debridement with local fragment / FB removal.
- Strong possibility of significant blood loss. strong consideration to initiate resuscitation with 1:1:1 PRBC:FFP:Plt or whole blood prior to or at the start of surgical intervention.
- Tailor decompression to fit the area of injury if possible.
- Avoidance of CSF leak is critical. Liberal use of CSF diversion.
Additional Assessment:
- Examination: Assess entry and, if applicable, exit wound. Ongoing neurologic assessment for lateralizing signs.
- Imaging: Review CT head for fragment/missile trajectory, determine lobes injured, assess for skull base/ vascular injury (see additional algorithms).
- Indications for surgery:
- Significant brain injury/mass lesion/edema requiring decompression
- CSF or brain contents extruding from entry/exit site
- Protruding foreign body (see foreign body algorithm)
- Concomitant skull base injury (see skull base algorithm)
- Concomitant vascular injury (see vascular injury algorithm)
Surgical TechniqueResuscitation: Anticipate significant blood loss. Depending on degree of injury, initiate resuscitation with PRBC:FFP:Platelets in 1:1:1 ratio in advance of or as starting operative intervention. Consider whole blood if available.
Incision/exposure: Account for area to be decompressed and repaired. Wide exposure to account for unanticipated pathology. Incision may or may not incorporate entry or exit site. Consider early harvest of vascularized pericranium as indicated.
Poorly designed incision results in inadequate exposure, inadequate decompression, poor wound healing.
Cranial Decompression: Account for trajectory of penetrating object and include injured brain. Must adequately decompress the brain in anticipation of significant swelling.
Inadequate or small decompression results in secondary brain injury.
Debridement: Remove superficial fragments, bone, hair, debris. Irrigate the trajectory cavity, but do not chase and remove deep fragments/debris/bone.
Removal of deep or indriven fragments results in additional brain injury.
Dural Repair: Leave dura open over the convexity, repair over skull base if possible. Utilize dural onlay substitutes or autologous materials (pericranium, fascia lata, etc.). Consider addition of dural sealants as appropriate.
Skin Closure/CSF Diversion: It is imperative that CSF leakage be avoided. In the absence of a watertight dural closure, water-tight galea/skin closure is imperative. Consider diverting CSF with ventriculostomy to both aid with ICP control and improve chances of incisional healing.
Poor skin closure or failure to divert CSF results in CSF leak and infection.
Delayed Considerations:
- Foreign body: Consider removal of foreign body if migration / infection noted on interval CT brain.
- Cranioplasty: Should be performed when safe and feasible. Consider delay if wound not completely healed or if evidence of infection.
Early cranioplasty results in infection. Migrating FB causes additional injury.