- Recommendations
CSF Leaks
Level IThere is insufficient evidence to support a strong recommendation related to infection risk and treatment of CSF fistulae following pTBI.
Level IICSF fistulae should be surgically repaired following pTBI to reduce the risk of infection and poor outcome.
Dural Repair Material
Level I - IVThere is insufficient evidence to support an evidence-based recommendation for dural repair by an allograft or autograft to prevent CSF fistulas.
Level C - Expert Consensus (Delphi Voting)In the absence of direct scientific evidence, EXPERT CONSENSUS concluded that:
- In the presence of a pTBI, it is recommended to prophylactically repair the violated dura directly or by application of an autograft (tensor fascia lata, pericranium, temporalis fascia) or allograft to prevent CSF leaks and prevent deep CNS infections and mortality. CSF drainage can be considered as an adjunctive measure. (93.3% consensus)
No evidence or expert opinion supported distinct recommendations based on patient gender, age, wounding mechanism, or military vs. civilian context.
- Introduction
The human brain is immersed in CSF which is tightly sealed by dura and leptomeninges while supported by the cranial vault and scalp. As such there is no free communication of subarachnoid space with the skin surface, paranasal sinuses and mastoid air cells. Penetrating traumatic brain injury (pTBI), being an open wound, violates this secure environment by two mechanisms.
1 Direct penetration of scalp and skull is followed by laceration of dura and pia-arachnoid resulting in CSF leakage and access of subarachnoid space by skin contaminants. Skull base penetration of paranasal sinuses and mastoid air cells results in rhinorrhea and otorrhea with added risk of backward extension of nosocomial contaminants into the intracranial cavity.2,3 Experience from multiple conventional military engagements has indicated that violation of the ventricular systems and basal cisterns make victims of pTBI particularly prone to CSF leakage and deep CNS infections.4 Whereas CSF leaks in blunt TBI have a high probability of healing with conservative management or with CSF diversion, CSF fistulae associated with pTBI are generally gaping and unlikely to resolve without surgical repair. - Prior Guidelines Recommendations
Management recommendations in the previous edition of these guidelines were provided on this topic at the level of options. This was based on 9 articles (seven military and two civilian GSWH). The recommendation stated that:
"Surgical correction is recommended for CSF leaks that do not close spontaneously, or are refractory to temporary CSF diversion. During the primary surgery, every effort should be made at close the dura and prevent CSF leak."
Since 2001 8 articles (six civilians and two military) provided a higher level of evidence than in the first edition, leading to a moderate strength recommendation in this edition.
- Scientific Foundation
We identified no comparative studies where some patients received planned water-tight dural closure and other patients received planned no dural closure or less-than-water-tight dural closure. We identified 16 non-randomized studies (N=6,452) that reported outcomes in patients where water-tight dural closure was attempted, though not always successfully. Mean sample size was 403 (range 13 to 1,732), average study mean age was 24.6 years (range 21 to 37.8 years) in studies that reported age (9 studies), average study proportion males was 94% in studies that reported proportion of males (11 studies). Eight studies were in a military population, six in a civilian population, and two in mixed military and civilian population. The vast majority of penetrating injuries involved gunshot wounds or shrapnel. Three studies were conducted in Vietnam and Turkey; two studies were conducted in the United States, Croatia, and Korea; one study each was conducted in Brazil, India, Iran, and Iraq. No specific harms of watertight closure of the dura were reported.
Four non-randomized studies (N=2,206) reported infection rates in the proportion of patients with cerebrospinal fluid (CSF) fistula compared with those without fistula.
5-8 - In a military pTBI population (N=379) from the Iran-Iraq War
5 , the authors reported watertight closure in all operative cases by the following means: primary closure (N=49, 13%), tensor fascia lata (N=288, 76%), and pericranium/temporalis fascia (N=41, 11%). In all patients in this series the dura was closed with 4-0 nylon monofilament suture and plastic surgeon assistance was utilized for complex scalp wounds. CSF fistulas occurred in 33 patients (8.7%). Of those, the most common locations were from the scalp (N=23), followed by orbit (N=7), nose (N=2), and ear (N=1). Twelve of the 33 patients (36%) developed central nervous system (CNS) infections compared with 1.7% (6/346) of patients without CSF fistula (p<0.001). Of patients with CSF fistula and positive CSF culture (50%), all were secondary to gram negative infections with Klebsiella pneumonia, Enterobacter, and/or pseudomonas aeruginosa. The authors also noted that they were forced to perform daily lumbar puncture, insert lumbar drainage catheters, or place shunts to prevent CSF fistulae in select cases and in some patients, reoperation that entailed re-suturing dural or scalp fistulas several times before CSF leaks ceased was required. However, no data were provided for these. Site of injury was not a contributing factor to rate of infection in this series. The major contributors to infection in this series were due to CSF fistula and gram-negative bacterial meningitis. There were no complications reported due to pericranium/tensor fascia lata/temporalis graft harvest and no complications attributed to watertight dural closure in this series. There were 32 total deaths in this series. Deaths due to infection occurred in seven patients (18 total infections, 38.8%). The mortality rate for gram negative bacterial infection was 71% (N=5/7). The rate of gram-negative bacterial infection was higher in patients with CSF fistulae (54%) than those without fistulae (16.6%). - From the Vietnam War 1,133 pTBI patients were studied.
6 The authors reported an incidence of CSF fistula of 8.9% (N=101). Of these, 54 (53.4%) occurred at the vertex/wound site, 30 (29.7%) with rhinorrhea, and 23 (22.8%) with otorrhea. Two cases presented with rhinorrhea and a wound site fistula, while four cases presented with both otorrhea and a wound site fistula. There were 28 patients with presumptive transventricular wounds who developed CSF fistulae. The infection rate of the entire cohort was 8.6% (97/1,133). Of patients with and without CSF fistulae, the rates of infection were 49.5% (50/101) and 4.6% (47/1,023), respectively. Of the patients with vertex/scalp CSF fistulae, 12 underwent initial attempted primary closure, 34 underwent grafted closure (graft type not described), two cases the closure type was unknown, and in six cases no closure of the dura was performed. Data for these patients were reported in aggregate. Of these patients (N=54), 57.4% (N=31) developed an infection. In the case of rhinorrhea 41.4% (12/30) developed an infection and for those with otorrhea 47.8% (11/23) developed infection. There were 11 patients in this series for which resolution of CSF leak was not achieved by surgery and they all died. The authors concluded that inadequate closure of the dura and scalp is a frequent cause of failure to prevent an infection. The mortality of patients with CSF fistulae was 22.8% (23/101) compared with 5.1% (53/1032) in patients without CSF fistulae. There were no adverse events reported secondary to graft harvest or watertight dural closure. - A cohort of 374 pTBI patients with missile head wounds were studied in Turkey. The authors reported infection rates associated with CSF fistulae in a mixed military/civilian cohort (N=374) of patients with penetrating injuries in Turkey.
7 All patients in this series underwent surgical intervention, which consisted of debridement and watertight closure of the dura by the following means: primary (N=59, 15.7%), pericranial/temporal fascia graft (N=285, 76.2%), tensor fascia lata graft (N=22, 5.9%), or cadaveric dural graft (N=8, 2.1%). Nineteen patients developed CSF fistulae in this series (5.1%), of these, 13 developed CNS infections (68.4%). There was one case of purulent ventriculitis (N=1/19, 5.3%), five cerebral abscesses (N=5/19, 26.3%), three subdural empyemas (N=3/19, 15.8%), three with cases of meningitis (N=3/19, 15.8%), and one superficial infection (N=1/19, 5.3%). This is contrasted with an incidence of infection in the cohort without CSF fistulae (N=5/355, 1.4%). In this group there were no instances of purulent ventriculitis, subdural empyema, or meningitis. There were four instances of cerebral abscess (80%, N=4/5) and one superficial infection (20%, N=1/5). There were no adverse events associated with watertight dural closure reported. -
A mixed military/civilian pTBI cohort of 288 patients were reported from Turkey. The fourth study also reported infection rates in the setting of CSF fistulae in a mixed military/civilian cohort (N=288) who underwent craniotomy, debridement, and watertight closure of the dura in Turkey.
8 Watertight dural closure was obtained by the following means: primary (15%, N=45), pericranial/temporal fascia graft (76.4%, N=220), tensor fascia lata (5.9%, N=17), and cadaveric dural graft (2.1%, N=6). The authors reported an incidence of CSF fistulae of 4.5% (N=13). There were 11 intracranial infections in the total study cohort with a majority occurring in patients with CSF fistulae (69.2%, N=9/13) compared with patients without CSF fistulae (0.73%, N=2/275). No adverse events of watertight closure or grafting were reported by the authors.
A pooled analysis of these four pTBI studies found a greatly increased risk of infection in the presence of CSF fistulae compared with no fistulae (relative risk 30.18, 95% CI, 14.34 to 63.53, Figure).5-8 This analysis provides moderate strength evidence that infection risk is greater when patients have a CSF fistula.
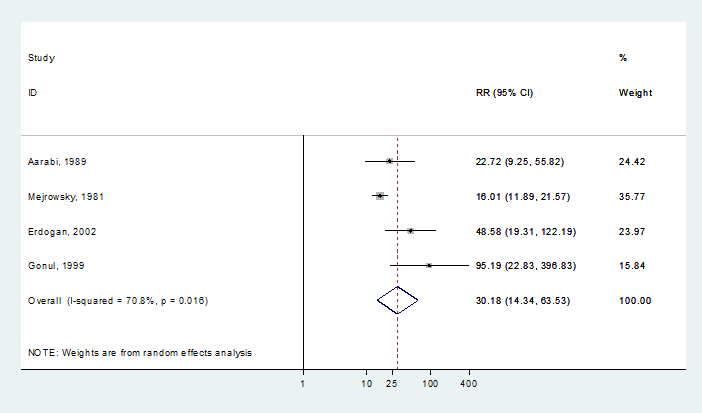 Pooled analysis of risk of infection in the presence of CSF fistula (CI=confidence interval; CSF=cerebrospinal fluid; RR=relative risk)
Pooled analysis of risk of infection in the presence of CSF fistula (CI=confidence interval; CSF=cerebrospinal fluid; RR=relative risk) - An additional cohort pTBI study (N=964) that also indicated a positive relationship between a CSF fistula and infection could not be added to the above analysis as raw data counts are not reported.
9 In this study, 54.8% had penetrating injuries (N=528) and 7.5% had perforating injuries (N=72) due to military conflict. Primary radical procedures, including watertight closure, were performed in 414 patients. Univariate analysis indicated an association of development of CSF fistula and infection (53.13%, x2=187.75, p<0.0001). On multivariable analysis development of CSF fistula remained associated with development of infection (Wald x2=46.5260, OR 11.931, p=0.0001). It should be noted that data for patients with watertight closure were reported in aggregate with patients for whom closure type was not available and variable treatments were performed for CSF fistulas including reoperation, lumbar punctures, and continuous CSF drainage. -
Another pTBI study that could not be added to the above analysis because there were no patients with a CSF fistula was in a population of military patients (N=60) in India.
10 Of 60 patients who were admitted with penetrating cranial wounds, 52 underwent acute surgical intervention including six who had previously undergone limited surgical procedures at forward operating bases. The authors reported that in all cases dural defects were closed with either a pericranial or temporal fascia graft to achieve a watertight closure. There were no CSF leaks in patients who underwent surgery and no patients developed brain abscesses. The authors attribute this to early surgical intervention (≤48 hours of injury) and the absence of CSF fistulae in this series. The average time to surgical intervention in this series was 36 hours post-injury (range 6 to 72 hours) and all patients were started on antibiotics within 6 hours of injury. There were no adverse events reported secondary to watertight closure of the dura.
The remaining 10 non-randomized studies reported other outcomes including rhinorrhea, otorrhea, reoperation, and overall mortality among others. These studies are further described below and in the table. Studies in a military population are presented first, followed by studies in a civilian population. - One study reported outcomes for a series of military patients with penetrating traumatic brain injury (pTBI) in the Vietnam War.
11 The study cohort was comprised of 103 patients with gunshot wounds to the head who underwent surgical intervention, however, complications were only reported for survivors (N=91). The authors implied watertight dural closure was performed in all cases and noted an incidence of CSF leak of 2.1% (N=2). In both cases, re-exploration identified an absent or misplaced dural suture at the primary closure site and determined this as the etiology of the leak. - A cohort of 312 pTBI was studied from Croatia reported surgical debridement and watertight dural closure in all patients when deemed appropriate.
12 The incidence of CSF fistula was 14.4% (45/312). The incidence of fistula for the entire cohort by site were: 4.8% (15/312) at wound site, CSF rhinorrhea 7.4% (23/312), and CSF otorrhea 2.2% (7/312). Of fistulae identified: 33% occurred at site of injury (15/45), 51% (23/45) were via the nose, and 15% (7/45) were via the ears. All patients with wound site fistulae underwent surgical intervention and three required subsequent reoperation for persistent leak. The authors utilized patch grafting with muscle, tensor fascia lata, or alloplastic material/lyophilized dura and fibrin glue. The incidence of postoperative meningitis was 13.3% in patients with CSF fistulae (6/45) and all instances occurred in patients with CSF rhinorrhea. It should be noted that it is unclear which patients underwent initial attempt at primary repair and which cases underwent a trial of spontaneous closure. It also should be noted that the cohort reported data in aggregate with 10 patients with closed head injuries. - A group of 62 military pTBI patients were reported from Croatia. Four patients had primary closure of the dura, 45 patients underwent watertight closure with grafts and 53 total procedures were performed in these patients.
13 The number of total procedures includes those with through and through/bilateral repair and eight patients who required reoperation. The authors separated the cohort into groups by graft type: fascia or temporalis muscle (Group 1), lyophilized dura (Group 2), periosteum (Group 3), tensor fascia lata (Group 4). Group 1 was comprised of only two patients and the mortality was 50%. Group 2 was comprised of six patients and mortality was 83.3% (N=5/6), and one patient developed CSF leak and meningitis. There were no intracranial infections identified on autopsy of those who died. Group 3 was comprised of 22 patients of which nine died (41%). Among those who survived there were three patients who developed CSF leak and meningitis, one who developed encephalitis, and three who required reoperation where periosteum was replaced with tensor fascia lata grafts. Among the nine deaths in this group there was one CSF leak and one instance of meningitis. Group 4 was comprised of 15 patients, four of whom died (mortality 26.7%). Among those who survived there were no CSF fistulas. Among those who died (N=4), there were two instances of CSF leak, wound dehiscence, and meningitis. There were no adverse events reported by the authors due to type of graft utilized for watertight closure. - One military pTBI cohort of 1,171 patients were reported from Vietnam by Hammon et al. Outcomes of operative cases in the U.S. military and 561 cases in Vietnamese patients with pTBI in which watertight dural closure was achieved "in almost all cases" by dural grafting with muscle, fascia, or pericranium from the operative area.
14 If sterile graft material was not available in the immediate exposed area the authors extended a limb of the incision and obtained tissue from another cranial site. The mortality of the operative U.S. military cohort was 9.74% (114/1,171). There were 104 deaths attributable to cerebral mortality (8.88%) in the U.S. military patients and 76 cerebral deaths in the Vietnamese cohort (13.55%). Postoperative CSF fistula requiring reoperation or additional surgery occurred in 0.63% of cases (N=11). Postoperative meningitis occurred in 0.63% of cases (N=11). There were no adverse events reported by the authors due to watertight closure or graft harvest. - Wallace and Meirowsky reported 540 military pTBI patients from Korean Compaign.
15 There were 167 transventricular wounds in this study cohort. Dural grafts were utilized for closure and a total of 590 grafts were utilized in the surgical cohort. There were 489 grafts inserted during primary craniectomy, 64 grafts inserted at secondary craniectomy/craniotomy, and in 37 instances grafts required reinsertion or replacement during secondary operations. The following grafts were used: tensor fascia lata (N=198), temporal/occipital fascia (N=186), pericranium (N=155), and gelfilm/fibrin film (N=27). CSF fistulas occurred in 49 patients, 41 cases required secondary surgical closure of a dural defect. There were 144 cases of secondary surgical site exploration and graft viability was recorded: viable graft (N=90), viable graft with visible defect (N=25), non-viable graft (N=20), and gelfilm failure/migration (N=9). The authors did not report any adverse events secondary to dural graft harvest or watertight closure. - Thirty-nine civilian pTBI patients were reported from Iraq looking for association with type of dural patch graft (pericranium vs. tensor fascia lata) and outcomes by the Glasgow Outcome Scale (GOS).
16 All patients underwent craniotomy or craniectomy with watertight dural closure by pericranium (64.1%) or tensor fascia lata (35.9%) graft. The authors reported an incidence of CSF leak of 12.8% in the entire cohort. There was no association with type of graft used for dural closure (p=0.7). Of the cohort of patients who developed CSF leak, 40% achieved a poor outcome and 60% achieved a good outcome. It should be noted that the authors utilized GOS for determination of quality of outcome, but no strict definition was provided. There were no reported complications secondary to graft harvest or watertight closure. - From Brazil a cohort of 110 civilian pTBI patients were reported to define the incidence of CSF fistulae following duroplasty and watertight dural closure.
17 The authors noted that duroplasty was performed in 73% (N=81) of patients in the cohort and indicated that watertight closure was attempted in all patients. The mortality of the cohort was 24.5% (N=27). Reoperation occurred in 8.2% of cases (N=9). Among 83 survivors a total of 15 patients developed CSF fistula (18%). No patients who expired developed CSF fistulae prior to death (p=0.0175). - One study from Turkey reported a single institution experience (N=442) with civilian pTBI over a 16-year period.
18 The authors reported that "in most cases" dura was closed primarily (15.1%, N=67). In cases where the dura could not be primarily closed, the authors performed duroplasty with pericranium or temporalis fascia (57%, N=252), tensor fascia lata (4.2%, N=19), or cadaveric dura (2%, N=9). The aggregate incidence of CSF fistula in this population was 4.5% (N=20) and was not stratified by closure type. There were no comparison groups and definitive closure attempt was implied in all cases. - Kim et al reported 13 patients with pTBI due to civilian gunshot wounds looking for CSF leaks following watertight dural closure.
19 The incidence of CSF leak was 15.4% (N=2) and both cases resolved with CSF diversion without infection. - Outcomes following civilian pTBI in the United States was studied by Sherman et al.
20 The authors report operative outcomes for 79 patients who underwent operative intervention for gunshot wounds. In all cases dural closure was attempted. The authors reported a rate of CSF fistula of 10.1% for the entire study cohort. No leaks occurred at the surgical scalp wound or vertex. There were seven cases of CSF rhinorrhea and one case of CSF otorrhea. In these eight cases, five leaks resolved spontaneously and two required reoperation for definitive closure. One patient died with a persistent CSF fistula. The authors reported no adverse events from dural closure. - In an epidemiologic cohort civilian pTBI study, Aarabi et al reported on outcomes for 192 patient who were admitted to nine trauma centers in Maryland over a two-year period.
21 Of the study cohort 15 patients underwent craniotomy with watertight dural closure. Of these patients there was one patient with CSF leak (CSF rhinorrhea) that required reoperation and dural repair and one epidural/subdural empyema that required washout. No description was provided for primary or grafted dural closure and no adverse events were reported secondary to watertight closure. Demographics for this subgroup were unable to be elicited. - From Balkan Campaign Tudor et al reported on their experience with CSF fistulae. In a military population with pTBI the investigators looked for an association of infection and reoperation with presence of a CSF fistula.
22 This study was not included as formal evidence nor included in the Table due to lack of surgical description or granularity with respect to closure or non-closure of the dura. However, this work is contained within the text due to the findings of: presence of CSF fistula was associated with development of infection. CSF fistula occurred in 11% of patients (N=21). Of patients without CSF fistula, 12% developed infections. Of patients with CSF fistula, 47.6% developed infection (x2=15.33, p<0.001). The authors also reported higher rates of reoperation in patients with CSF fistulae (76%) compared with patients with deep seated infections (60%, x2=43.6, p=0.00001) and patients without infections (8.4%, x2=56.95, p=0.00001). It should be noted that no clear description of reparable or non-reparable (craniobasilar injuries) were given for this patient population. The authors defined watertight dural closure as "not allowing a CSF fistula to develop."
Several other works were identified that support the above findings, but did not meet criteria for inclusion due to lack of granularity of injury patterns or procedures performed,
23 or no clear description of dural closure were provided (watertight, primary-repair, onlay only, combination).24,25 One study was identified in a population of U.S. military patients that concluded that watertight closure, harvesting adjunct grafts (pericranium), or utilizing suturable grafts was time consuming and noted benefits were not apparent relative to the increased operative time in multiply injured patients.
26 However, no objective measures were provided supporting this claim.There were no harms reported secondary to watertight closure or associations with type of dural graft used.
- In a military pTBI population (N=379) from the Iran-Iraq War
- Discussion
KH was a 36-year-old lady who attempted suicide following years of depression (Fig1). The slug penetrated the left orbital apex and ethmoid air-cells before tearing into the dura mater and left frontal lobe. The fragment lodged into the vertex parietal bone after ricocheting near the coronal suture. At the time of admission (May 10, 2015) she was stuporous (GCS 7, motor score 5) with frozen left-eye movements and a dilated and nonreactive pupil. There was right sided hemiparesis. Computed tomography depicted the site of penetration near left medial orbital wall, orbital roof, frontal skull base, left frontal lobe in conjunction with an acute subdural hematoma and shift of the midline structures to the right side (Fig 2, plates A, B, C, and D). Digital subtraction angiography did not reveal any vascular injury (Fig 2 plate E). An urgent decompressive hemicraniectomy was followed by CSF diversion and external ventricular drainage (Fig 2 EVD, plate F). Postoperatively, free flow of CSF and pulped brain was noticed from the soft palate and nostrils. The patient was re-explored, primarily repairing the frontal base dural defect followed by reconstructing the perforation near the left orbital roof (Fig 2 plates G, H). Six weeks following her pTBI injury the patient had autologous cranioplasty (Fig 2 plates I and J). Three months following pTBI she was alert and oriented but had left eye blindness and moderate weakness of right foot.
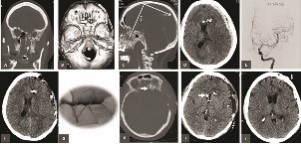 Figure 1: Mugshots indicating the mechanism of pTBI in a 36-y-o lady who attempted suicide by a submental GSWH.
Figure 1: Mugshots indicating the mechanism of pTBI in a 36-y-o lady who attempted suicide by a submental GSWH. Figure 2: Coronal, basal, sagittal and axial CT cuts indicating entrance and ricochet of the bullet causing acute subdural hematoma on the left side (plates A, B, C, D). Digital subtraction angiography of left carotid (plate E), Post-operative axial CT cut post decompressive craniectomy (plate F), intraoperative sketch indicating primary repair of dura (G) and multiple axial CT views of post-op course up to cranioplasty (plates H, I and J).
Figure 2: Coronal, basal, sagittal and axial CT cuts indicating entrance and ricochet of the bullet causing acute subdural hematoma on the left side (plates A, B, C, D). Digital subtraction angiography of left carotid (plate E), Post-operative axial CT cut post decompressive craniectomy (plate F), intraoperative sketch indicating primary repair of dura (G) and multiple axial CT views of post-op course up to cranioplasty (plates H, I and J).Cerebrospinal fluid leaks are the scourge of pTBI management and have to be taken seriously. The best evidence for this statement is not only the findings from the preceding literature review but also by considering the history of pTBI management.
27 Mortality/morbidity due to infection was appallingly high during the "Pre-Modern Era" of neurosurgical techniques in management of missile head wounds, which coincided with the end of the American Civil War in 1865.27 The introduction of asepsis, antiseptics, and anesthesia during the "Modern Era, 1865-1918" combined with meticulous debridement of the pTBI track and watertight closure of scalp by Cushing reduced infection rate to 35 percent.4,27,28 A simple comparison of Cushing's work with that of Whitaker who left the entrance wound of pTBI open indicates higher rate of mortality in the latter surgeon's surgical technique precipitated by deep CNS infections.4,28,29 It was Cushing's suggestion that penetration of the ventricular system was important in CSF leaks predisposing to meningitis and ventricultitis.4,28,30 The significance of CSF leaks and their relationship with deep CNS infections was taken very seriously during the Second World War as expressed by Ascroft and Cairns.2,31-35 The relationship between CSF fistulas and orbitofaciocraniocerebral injuries, involvement of basal cisterns and cerebral ventricles was further confirmed during the Second World, Korean, Vietnam Wars, and Middle Eastern Conflicts.36-39 The fact that pTBI is the mother of all CSF leaks and the building block of deep CNS infections is clearly supported by Class II evidence collected from multiple conflicts starting from WWI4,28,29 to WWII2,31,35 , Korean Conflict,3,40 Vietnam War41 and Middle East Campaigns.5,36,42,43 and our Consensus Delphi conference recommends repair of this pathologic entity by any means including primary repair, allo- or autograft. CSF diversion can be considered an adjunct in such repairs. - Expert Opinion
Harvey Cushing was first to recommend watertight closure of scalp in order to prevent CSF leaks especially if basal cisterns or the ventricular systems were violated.
4 Subsequently it was learned that in the majority of cases with pTBI the hot projectile not only will cut the dura, it will cause retraction of the latter with less chance to be repaired primarily.5 During WWII, Korean, Vietnam, Middle East and Balkan conflicts we experienced the need for a fascial dural graft in order to prevent CSF leakage - especially in lacerations of basal dura, in order to prevent CNS infections.1,31,36,44-47 Based on this low level evidence, the Delphi Consensus decision was to recommend dural graft in the majority of patients with dural laceration in order to prevent CSF leaks and CNS infections. - Future Directions
Level II evidence supports a moderate strength recommendation that CSF fistulas predispose the victim of pTBI to deadly CNS infections and that they should thus be prevented. Future prospective observational studies should clarify if allografts (Lyodura, Dura Guard, Duraflex) are as effective as autografts (pericranium, temporalis fascia, tensor fascia lata) in preventing CSF fistulas and CNS infections, and what their relative risk for infection is.