Inadequate exposure results in incomplete skull base repair.
- Penetrating Skull Base Injury Toolkit
Penetrating skull base injury is not the same as a skull base injury associated with closed head injury. Accepted management of cerebrospinal fluid leakage in the setting of skull base injury or disruption associated with closed head injury may include a period of observation to determine if the leak will seal without intervention
104,105 . This will likely not occur in penetrating skull base injury, especially with penetration through air sinuses. It is the opinion and experience of the current authors that significant delay in repair will simply guarantee infection and not resolution. With this in mind, penetrating skull base injury repair should occur as soon as safe and feasible (i.e., assembly of appropriate operative resources including multi-disciplinary expertise (plastic surgery, ENT/OMFS, ophthalmology)106,107 as appropriate; associated cerebrovascular injury diagnosed and potentially addressed). In the authors' experience, it is the anterior fossa that is most often injured, followed by middle fossa injury through the lateral wall of the sphenoid sinus.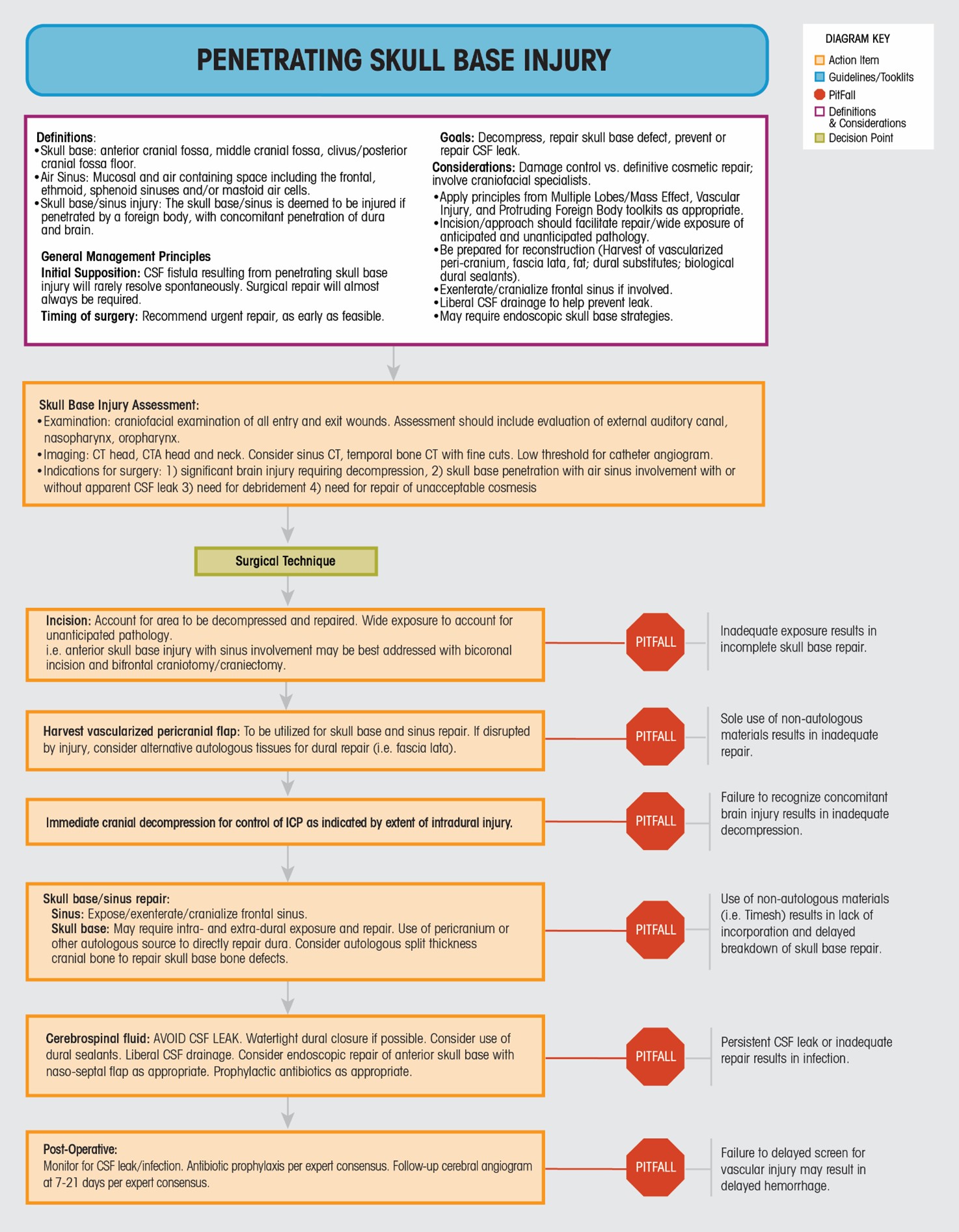
It is beyond the scope of this algorithm to address the specific technical nuances of individual skull base approaches and repair techniques. The following will address the main areas that should be considered during penetrating injury repair. The goals of surgery remain first and foremost cranial decompression and control of hemorrhage, followed by skull base repair and prevention of cerebrospinal fluid leak. Patient positioning and operative exposure should therefore account for the location of the skull base injury, and the possible need for cerebral decompression. Harvest of a large vascularized pericranial flap during exposure adds little time to the procedure and can facilitate adequate repair. Assuming adequate cranial decompression without rapid and malignant swelling, it is then necessary to approach the area of skull base disruption. Exenteration and cranialization of the frontal sinuses may be necessary if the anterior fossa is disrupted. Approach to orbital or ethmoidal penetrating injury may include an intra- and extra-dural exposure, and may also require endoscopic augmentation with naso-septal flap or other techniques
107-111 . If significant bone disruption is present, repair with autologous (split thickness) cranial bone is preferable over synthetic materials (i.e. timesh). Most importantly, every effort should be made to avoid CSF leak, including the use of dural sealants, primary dural closure where possible, and cerebrospinal fluid diversion. The importance of achieving a water tight dural closure takes precedence over the desire to avoid the use of synthetic materials or devascularized tissues within a contaminated wound in this context. Broad spectrum antibiotic coverage, depending on the wounding mechanism and degree of contamination, will likely be necessary for a period of time. - Penetrating Skull Base Injury ToolkitPenetrating Skull Base Injury
Definitions:
- Skull base: anterior cranial fossa, middle cranial fossa, clivus / posterior cranial fossa floor.
- Air Sinus: Mucosal and air containing space including the frontal, ethmoid, sphenoid sinuses and/or mastoid air cells.
- Skull base/sinus injury: The skull base/sinus is deemed to be injured if penetrated by a foreign body, with concomitant penetration of dura and brain.
General Management Principals:
Initial Supposition: CSF Fistula resulting from penetrating skull base injury will rarely resolve spontaneously. Surgical repair will almost always be required.
Timing of surgery: Recommend urgent repair, as early as feasible.
Goals: Decompress, repair skull base defect, prevent or repair CSF leak.
Considerations: Damage control vs. definitive cosmetic repair, involve craniofacial specialists.
- Apply principles from Multiple Lobes/Mass Effect, Vascular Injury, and Protruding Foreign Body toolkits as appropriate.
- Incision/approach should facilitate repair/wide exposure of anticipated and unanticipated pathology.
- Be prepared for reconstruction (Harvest of vascularized peri-cranium, fascia lata, fat; dural substitutes; biological dural sealants).
- Exenterate / cranialize frontal sinus if involved.
- Liberal CSF drainage to help prevent leak.
- May require endoscopic skull base strategies.
Skull Base Injury Assessment:
- Examination: craniofacial examination of entry and exit wounds. Assessment should include evaluation of external auditory canal, nasopharynx, oropharynx
- Imaging: CT head, CTA head and neck. Consider sinus CT, temporal bone CT with fine cuts. Low threshold for catheter angiogram.
- Indications for surgery:
- significant brain injury requiring decompression
- skull base penetration with air sinus involvement with or without apparent CSF leak
- need for debridement
- need for repair of unacceptable cosmesis
Surgical TechniqueIncision: Account for area to be decompressed and repaired. Wide exposure to account for unanticipated pathology.
i.e. anterior skull base injury with sinus involvement may be best addressed with bicoronal incision and bifrontal craniotomy / craniectomy.
Harvest vascularized pericranial flap: To be utilized for skull base and sinus repair. If disrupted by injury, consider alternative autologous tissues for dural repair (i.e. fascia lata).
Sole use of non-autologous materials results in inadequate repair.
Immediate cranial decompression for control of ICP as indicated by extent of intradural injury.
Failure to recognize concomitant brain injury results in inadequate decompression.
Skull base/sinus repair:
Sinus: Expose / exenterate / cranialize frontal sinus.
Skull base: May require intra- and extra-dural exposure and repair. Use of pericranium or other autologous source to directly repair dura. Consider autologous split thickness cranial bone to repair skull base bone defects.
Use of non-autologous materials (i.e. Timesh) results in lack of incorporation and delayed breakdown of skull base repair.
Cerebrospinal fluid: AVOID CSF LEAK. Watertight dural closure if possible. Consider use of dural sealants. Liberal CSF drainage. Consider endoscopic repair of anterior skull base wth naso-septal flap as appropriate. Prophylactic antibiotics as appropriate.
Persistent CSF leak or inadequate repair results in infection.
Post-Operative:
Monitor for CSF leak/infection. Antibiotic prophylaxis per expert consensus. Follow-up cerebral angiogram at 7-21 days per expert consensus.
Failure to delayed screen for vascular injury may result in delayed hemorrhage.