- RecommendationsLevel I - IV
There is insufficient evidence to support an evidence-based recommendations for a multidisciplinary team surgical approach in patients with facio-orbito-craniocerebral injuries.
Level C - Expert Consensus (Delphi Voting)In the absence of direct scientific evidence, EXPERT CONSENSUS concluded that:
- When accessible, a multidisciplinary teamwork approach to surgical management of pTBI involving face, orbits and frontal skull base is recommended. (100% consensus)
- If a multidisciplinary approach to surgical management of pTBI involving face, orbits and skull base is not immediately feasible, life-saving damage control surgical procedures followed by transfer to a center with available multidisciplinary teams is appropriate when able. (100% consensus)
No evidence or expert opinion supported distinct recommendations based on patient gender, age, wounding mechanism, or military vs. civilian context.
- Introduction
Penetrating TBI involving the face, orbits and cranium
1-3 is a devastating phenomenon that requires capable surgeons to repair the disfigurement of the face, cranium and orbits while simultaneously preventing cerebrospinal fluid (CSF) leakage through the air sinuses. Often these injuries involve facial and orbital repairs outside of traditional neurosurgical training, and therefore plastic, oromaxillofacial and ophthalmological surgeons are also needed.These injuries may involve the face and orbits alone, but when pTBI is present, the neurosurgeon has a vital role in the reconstruction of the anterior skull base and prevention/treatment of CSF leakage through the air sinuses. The mechanism may involve low velocity injury penetration such as present with the knife
4 , blast injuries as are seen frequently in military conflict,5-7 or civilian injuries.4 One common civilian injury is submental or transoral, self-inflicted gun shot wounds.1, 2 As the trajectory involves the face, eyes, and brain, a multidisciplinary approach is essential. - Prior Guidelines Recommendations
The prior pTBI guidelines did not endeavor to address this topic.
- Scientific Foundation
We identified no studies that compared a multidisciplinary with a single-disciplinary approach to penetrating traumatic brain injury (pTBI) surgery or management. However, we identified several noncomparative studies that reported using a multidisciplinary team.
1-3 As there were no comparative studies, all recommendations we provide are based on expert consensus.One retrospective database by Stephens et al
5 reviewed 108 injuries from Operation Iraqi Freedom and Operation Enduring Freedom (Afghanistan) who underwent a decompressive craniectomy and subsequent cranioplasty.5 Ninety-three (86%) had a penetrating injury primarily due to an explosive blast. Repairing the soft tissue and skull base required a multidisciplinary team consisting of neurosurgery, reconstructive plastic, oral-maxillofacial, and ophthalmologic surgery that was individualized for each patient. One patient died (0.93%). Other complications included infection (12%), seizure (7.4%), and extra-axial hematoma (7.4%).A study by Elegbede et al
1 of 69 patients with a self-inflicted gunshot wound to the face (submental [57%], intraoral [22%] and temporal [12%]) reported multispecialty surgical management including facial reconstructive surgery (57%), ophthalmology (14%), and neurosurgery (26%). Additionally, 33% required a tracheostomy and 38% required a gastrostomy. Twenty-eight (41%) had a GCS score greater than 8 at baseline. Eighteen patients died (26%). However, only 41% of the patients (N=28) sustained a pTBI.Another combat study by Weichel et al
3 of 152 casualties from Operations Iraqi Freedom and Enduring Freedom experienced 207 globe/oculoplastic injuries and were treated by ophthalmology, as well as other medical and surgical specialties. However, only 14% had pTBI. Mortality and vision loss were not reported in this study.One study by Kim et al
4 of 82 patients with craniofacial impalement injury by a metallic object used a multidisciplinary team (otolaryngologists, neurosurgeons, ophthalmologists, plastic surgeons, and anesthesiologists) for the removal of the foreign body under general anesthesia at two craniomaxillofacial trauma centers. Items of impalement in the eight patients included a saw wheel, knife, metal plate, and iron bar. Complications in these eight patients included one brain abscess, chronic pain, pseudoaneurysm, and hypertrophic scaring.One study of 11 patients by Kriet et al
2 with self-inflicted submental and transoral gunshot wounds and brain injuries were treated by neurosurgery, ophthalmology, and otolaryngology. Ophthalmological and craniomaxillofacial injuries were addressed following frontal craniotomy. One person received only supportive care and died. Complications for the other 10 patients included: cerebrospinal fluid leak, delayed frontal lobe infarction, scalp wound dehiscence, and extradural abscess.We found evidence that a multidisciplinary team is sometimes available and employed. However, we found no evidence to determine whether care from a multidisciplinary team results in superior or inferior outcomes when compared with care from a single-disciplinary team. However, consensus among experts with experience with these patterns of injury recommend a multidisciplinary approach when available or transfer to a center with these capabilities after medical stabilization and damage control surgery if needed.
- Discussion
Self-inflicted gunshot wounds and blast injuries can frequently involve submental, intraoral and trans-temporal regions, causing injury to the face, orbits, air sinuses and frontal skull base. These injuries may occur in civilian or conflict environments and may be low velocity pTBI, gunshot wounds, or blast injuries.
1,2,4,5 Blast injuries especially may involve multiple fragments penetrating the skull base secondary to the location of the exploding device. These injuries are extremely complex but are also survivable.1,2,5 Therefore, whether received in casualty clearing stations near the front-line or in a civilian hospital, every-effort should be made to bring together multispecialty surgeons in order to simultaneously repair the sub-frontal dura defect, air sinuses, orbital roofs and facial soft-tissue structures.If immediate, simultaneous repair is not possible, damage control surgical and medical interventions are appropriate followed by timely definitive surgical repair with a multispecialty team to avoid increased risk for infection. Often, transfer to another facility may be necessary after stabilization in both conflicts and civilian environments.
The multidisciplinary nature of these conditions extends beyond the surgical repair (Fig1). As the trajectory of the penetrating object often involves the superior sagittal sinus, anterior cerebral arteries, and potentially the basal cisterns, involvement of neurovascular and endovascular experts is often required as well. However, vascular injuries in pTBI are addressed in other aspects of these guidelines. Rehabilitation specialists are also required as well to achieve best outcomes. Rehabilitation not only helps to build muscle and adaptive strategies, it stimulates brain plasticity as well as other type of neural repair.
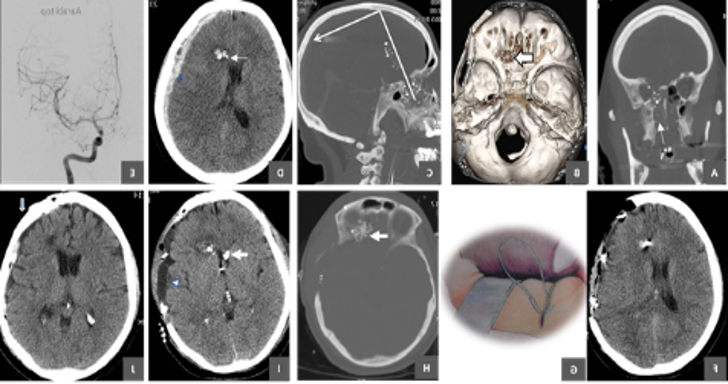 figure 1: 35-y-o lady who attempted suicide by an intra-oral GSW with slug penetrating hard palate, passing through the left medial orbital apex and ethmoids at the frontal skull base. The projectile ricocheted the frontal bone and was stopped by the parietal vertex. She was stuporous and her left pupil nonreactive to light. CT scan showed acute SDH and DSA negative for TICA. She had urgent decompressive craniectomy followed by repair of base dura and orbital roof during a second stage surgery in cooperation with ophthalmic surgeons after leakage of pulverized brain and CSF was noticed from her left nostril. The patient had cranioplasty 3 months following the pTBI. Six months following the suicide attempt she was blind in left eye and had 4/5 weakness of right eye.
figure 1: 35-y-o lady who attempted suicide by an intra-oral GSW with slug penetrating hard palate, passing through the left medial orbital apex and ethmoids at the frontal skull base. The projectile ricocheted the frontal bone and was stopped by the parietal vertex. She was stuporous and her left pupil nonreactive to light. CT scan showed acute SDH and DSA negative for TICA. She had urgent decompressive craniectomy followed by repair of base dura and orbital roof during a second stage surgery in cooperation with ophthalmic surgeons after leakage of pulverized brain and CSF was noticed from her left nostril. The patient had cranioplasty 3 months following the pTBI. Six months following the suicide attempt she was blind in left eye and had 4/5 weakness of right eye.Following review of the literature, no studies were found that compared a multidisciplinary with an isolated neurosurgical approach to pTBI of the face and orbits. As facial and orbital/eye repair is outside of the traditional training of most neurosurgeons, effective surgical treatment of these injuries is only possible through multidisciplinary teams. Although multiple individual operations are possible from each service, this approach carries the risk of multiple anesthetic administrations, increased risk of infection from additional operations, and potential disruption of previous surgical repair. For example, access to the orbit and forehead after cranialization of the frontal sinus could potentially de-vascularize the pericranial graft and threaten the CSF leak repair.
- Expert Opinion
In modern medicine, multidisciplinary care is essential to achieving best outcomes. pTBI patients can be extremely complex requiring the expertise of multiple medical and surgical disciplines. Therefore, a multidisciplinary teamwork approach to surgical management of pTBI involving face, orbits and frontal skull base is recommended. If these teams are not available, transfer to an appropriate facility with these services after medical and surgical stabilization is also recommended. Even the neurosurgical care may require the involvement of multiple neurosurgeon subspecialists such as those with advanced trauma, vascular, skull base and spine training.
- Future Directions
While the benefits of multidisciplinary care are obvious, evidence supporting this premise would be a valuable addition to the literature research. However, the impact of delays from presentation to definitive repair would certainly benefit from further study. This delay involves both transfer of the patient to facilities with all services available as well as finding operating room and surgeon availabilities as these cases can be long in duration. Increased wait times likely increase the risk of infection as CSF leakage is often present and the environment involves the nonsterile sinus mucosa. Therefore, further research on how time to definitive operative repair influences outcome is needed.