- Master Care Pathway
Care of patients with pTBI starts in the pre-hospital setting at the point of injury
9 . Emergency medical personnel responding to the scene are often faced with varying degrees of external injury and overall scene safety. Application of ATLS principles including initial focus on airway (with cervical spine protection), breathing, and circulation/hemorrhage control, is critical. Immediate transport to the nearest capable trauma center is either preceded or accompanied by immediate notification to the trauma center. Notification to the on call neurosurgical team is also recommended at this time. A protruding foreign body should not be removed outside of the controlled environment of an operating room or angiography suite (Section VI-2, On Scene Wound Care-Consensus Based Recommendation).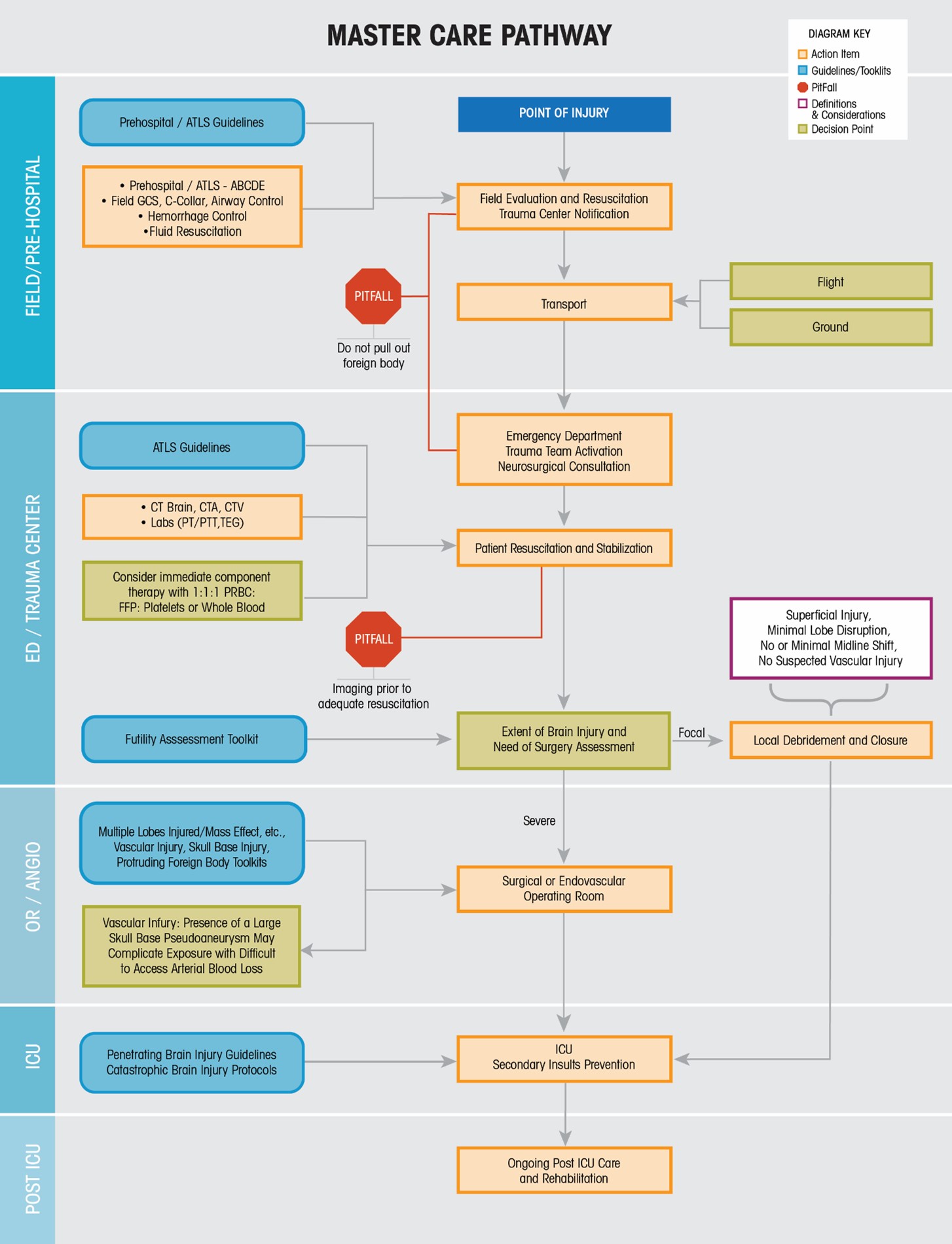
Upon arrival to the hospital, immediate ATLS guided re-evaluation is necessary, with simultaneous laboratory and image-based analysis. Attention to the ABCDEs with rescuscitation is the initial management priority. ATLS protocols must be followed strictly - the striking nature of pTBI can distract physicians and lead to deviations - this must be avoided. During the primary and secondary surveys it is crucial to identify the entry, and if present, exit wound, with consideration for multiple penetrating injuries and injured organ systems. Beware of nail gun injuries which are often occult as well as stab wounds where the penetrating implement has been removed. In severe cases, significant skull disruption is often encountered, with notable egress of injured brain, blood, and cerebrospinal fluid from a defect in the scalp. It is recommended that compressive dressings be avoided in this setting. The wound should not be probed and brain or other damaged tissue should not be debrided at this point (Consensus Based Recommendation, Section VI-2; On Scene Wound Care). Immediate neurosurgical consultation is recommended to assist with initial examination. When the patient is sufficiently resuscitated and it is judged safe to send the patient for imaging, this imaging should consist of immediate CT and CTA of the head and neck. Both are strongly recommended (Evidence Based Recommendations, Section VI-3, Diagnosis of ptBI; Level IV) and every effort to avoid delay is recommended. As CT imaging can be subject to scatter, skull x-rays continue to have a limited role in demonstrating the presence and location/trajectory of radio-opaque foreign bodies. Recognize that some foreign bodies like glass, wood and some rocks may be radiolucent, requiring MR imaging if it is felt that can be done safely (Section VI-8, Safety of MRI-Consensus Based Recommendation). Strong consideration for additional imaging including cerebral angiography may be considered at this point if traumatic vascular injury including traumatic aneuryms are noted on CTA (Section VI-6, Neurovascular Imaging, Evidence and Consensus Based Recommendations; Section VII-6 Endovascular Coiling of Traumatic Aneurysms, Evidence and Consensus Based Recommendations; See Traumatic Vascular Injury Toolkit)
10-20 . In addition to standard laboratory analysis including blood type and cross-match, viscoelastic testing can be helpful to ascertain precise coagulation abnormalities and to help guide specific corrective measures (Section VIII-1, Viscoelastic Testion, Evidence and Consensus Based Recommendations)21 . Additional resuscitation, including component (1:1:1) or whole blood transfusion is often necessary, and should begin immediately in patients with other than minimal injury in anticipation of the expected blood loss from operative intervention.At this point, all information gathered should be synthesized in preparation for additional decision making. It is strongly recommended that the clinician/neurosurgeon base decisions on medical futility at this time rather than short or long term prognosis or eventual functional outcome. We accepted the definition of medical futility as "A proposed therapy should not be performed because available data show that it will not improve the patient's condition"
22 . Futility is also distinct from the notion of survivability, which we viewed as the potential for a patient to survive if treated aggressively. The remainder of the algorithm defines patient movement through the hospital environment, with notable reminders concerning care provided in each location. - Master Care Pathway