- RecommendationsLevel I - III
There is insufficient evidence to support a strong, moderate strength or weak recommendation related to primary local wound debridement and closure in patients with pTBI.
Level IVLocal wound debridement is appropriate in patients with penetrating brain injury with good neurological status, minimal brain and soft tissue disruption as well as minimal wound contamination.
Level C - Expert Consensus (Delphi Voting)In the absence of direct scientific evidence, EXPERT CONSENSUS concluded that:
- In demanding circumstances such as mass casualties, in a conscious patient with penetrating brain injury and no intracranial bleeding, wound debridement and careful closure of a scalp laceration is recommended. (90% Consensus)
- It is recommended that casualties undergoing local wound debridement and closure be treated with short-term antibiotic(s) and have computed tomography (CT) scan of the head between 3-6 weeks to rule out abscess formation at the site of the penetrating projectile. (96.7% Consensus)
No evidence or expert opinion supported distinct recommendations based on patient gender, age, wounding mechanism, or military vs. civilian context.
- Introduction
Penetrating traumatic brain injury (pTBI) is by default an open wound with a tendency to expose intracranial structures as well as the cerebrospinal fluid to infectious organisms. It has therefore been the common perception of trauma surgeons that there is a need to debride the tract and close the dura water-tight and repair the scalp.
1-5 In 1991, however, during the Lebanese Civil War, Taha6 treated 32 patients by simple wound closure and reported an acceptable risk of infection and CSF leakage. This has led to a consideration of circumstances in which local wound debridement and closure may reasonably be performed or perhaps even preferred with a view that this finding may be relevant to both military and civilian care environments. - Prior Guidelines Recommendations
In the first edition of these guidelines this topic was discussed in the surgical section under the title "Less Aggressive Debridement in Military Circumstances". This concept ranged from simple wound closure to very superficial debridement.
6-11 Only Taha et al6 reported simple wound closure in 32 patients of which one patient developed a brain abscess following surgery. Since 2001, four non-randomized studies12-14 have been added to the literature. - Scientific Foundation
For this key question we included studies reporting local debridement and closure of wounds performed in an emergency room, at bedside, or in the field, but not in an operating room as part of a surgical intervention. We also included studies where this was presumed to be curative treatment and excluded studies where local debridement and closure were used only for patients not expected to survive.
There were no randomized trials or prospective cohort studies identified that addressed the benefits and harms of local debridement and closure as treatment for penetrating traumatic brain injuries (pTBIs). We identified five studies meeting inclusion criteria that provided information about patient outcomes and the indications for this treatment strategy, including one retrospective cohort study that compared outcomes for patients who received simple wound closure with those who received surgery
12 and two studies where all patients received local debridement.One nonrandomized study
12 reported by Krueger et al viewed all cases of gunshot wounds to the head from a single large trauma center in Florida from 2008 through 2018. Included patients were civilians older than 18 years of age who sustained a new, acute gunshot wound with suspected or confirmed dural penetration. Patients were excluded if they were transferred from other hospitals; had injuries that were not from a firearm; did not survive initial resuscitation; had an initial Glasgow Coma Scale (GCS) score of 3 or 4 and nonreactive pupils; or died or had confirmed brain death within 48 hours of admission. Sixty-seven patients were included: 17 were treated with simple wound closure (described in the Table) and 50 with surgery. The neurosurgeons made the treatment choice. The patients were clinically different: those who received surgery had a statistically significantly higher incidence of mass effects and involvement of frontal sinuses. While not statistically significant, the surgery patients had a lower mean GCS and more had fixed pupils. While this suggests the operated patients had more severe injuries, their outcomes, including mortality, Glasgow Outcome Scale-Extended (GOS-E) at 30-, 60-, and 90-days, infections, cerebrospinal fluid (CSF) fistulas, and seizures, were not significantly different. However, it is important to note that six (35.3%) of the patients who received simple wound closure and 14 (28%) who received surgery were lost to follow-up, and their results could change the conclusions in a study this size. In addition, the sample size may not provide sufficient power to detect clinically important differences.A case series from Amirjamshidi et al
14 reported long-term follow-up data on 99 patients of 191 victims of the Iran-Iraq conflict who were treated at two centers affiliated with Tehran University of Medical Sciences.15 These patients ranged in age from 13 to 55 years and all were male. Patients received no initial surgical interventions for pTBIs obtained in battlefield areas due to shrapnel and shell fragments. Patients who had a GCS score of 8 or higher, no rapid deterioration in consciousness, and a small entrance wound of less than 2 to 3 cm were candidates for local treatment. Patients were treated with wound cleaning, local debridement, stitches, and dressing at a field hospital. They were then transferred to a medical center where better X-rays and computed tomography (CT) scans were taken and cases were reviewed by the attending surgeon. Sixty-two cases had CSF leakage, or the wound was under tension, requiring more superficial debridement of the skin, bone, and any contused brain tissue; however, the attending surgeon determined more extensive debridement was not necessary. Patients were then admitted, treated with antibiotics for 2 weeks, and had at least two additional CT scans. Mean follow-up was almost 8 years, in which time 91% of patients had good outcomes and were able to perform their usual job/activities, 4% were severely disabled, and 5% had died of their injuries or meningitis. None of the patients had brain abscesses, epilepsy, or hematomas. Outcomes were not significantly different for the 37 patients who did not require additional superficial debridement after transfer compared with the 62 patients who did.In a another series reported by Taha et al
6 , 32 patients from conflict zones in Lebanon with shrapnel (84%) or gunshot injuries (16%) were treated within a mean of 3 hours after injury6 , in an emergency room, with superficial entry wound debridement and wound closure without drainage. Patients had to have a GCS greater than 10, an exam within 6 hours of the injury, a small entry wound, no exit wound, and to meet other criteria related to missile tract and hematomas (Table). Patients ranged in age from 3 to 51 years with a mean age of 32 years. Most (19 of 32) patients had an initial GCS of 15. At follow-up (mean 3.5 years after injury) there were no deaths and no neurological deficits. Only one patient (3.1%) had complications including a seizure and then a brain abscess that was excised; however, 2 months later the patient had no abnormalities.In two other studies, the cases were defined by the mode of injury, but the majority of patients were managed with local debridement and closure.
13,16 Kadhim et al13 in a non-randomized study reported care and outcomes for 30 patients treated for injuries from falling bullets, when guns are shot into the air often as part of celebrations. The patients were treated at one teaching hospital in Baghdad, Iraq.13 Patients ranged in age from 7 to 55 years with a median age of 17.5 years and 63% were male. Two thirds (66%) had an initial GCS of 13 to 15, and in another 10% of patients their initial GCS was 9 to 12. Nineteen patients were treated with local wound care, five had extra cranial bullets extracted, and six needed extensive surgery. Local wound care was the standard treatment unless a bullet caused a depressed skull fracture or indriven bone chips. Follow-up was limited to 6 months after hospitalization. At follow-up, 42% of patients who received local wound care had a Glasgow Outcome Scale (GOS) score of 5 (good recovery). Twenty-six percent (5/19) were GOS 4 (moderate disability) including patients with initial GCS of 4, 5, 8, 13, and 14. Two patients (11%) had a GOS 3 at the end of follow-up. Four patients died (21%), but it is important to note these patients all had an initial GCS of 5 or 6.Another series from Suddaby et al
16 from one hospital in Canada, included 49 patients treated for .22 caliber gunshot wounds.17 These were predominately suicide attempts (88%). The mean age of the patients was 30.4 years old, but they ranged from 9 to 92 years old and 88% were male. Patients were assessed in the emergency department and 36 were provided local wound care and then admitted, while 13 were taken to the operating room for surgical interventions. Unfortunately, the study authors did not report patient outcomes separately by type of treatment. We have included the outcomes and the study in the Table as it was included in the prior guideline and to highlight that this study included patients who were more seriously injured (64.5% have GCS ≤7) and had a much higher mortality rate (61%). However, as the results are not separated, we did not include it in our assessment of the strength of the body of evidence.One nonrandomized study and three case series provide very low strength of evidence that local debridement and closure are associated with good outcomes for appropriate patients.
12-14,16 However, the rigor of the studies limits and little information is provided on potential harms. The small number of studies/reports suggest that there may be publication bias, as it is at least possible that this approach to care has been tried more frequently, likely out of necessity, but that negative results may not have been published. - Discussion
In military or civilian pTBI from low velocity shell fragments (figure 1) or shot gun pellets (figure 2), as described in the report by Kadhim et al,
13 the foreign body carries at least 70 joules (J) energy18 , enough to lacerate scalp, penetrate skull and enter the brain without causing a temporary cavity. In Carey's feline experimentations, ordinary pressure waves with a magnitude of several atmospheric pressure were needed to produce temporary cavities.19 Under such circumstances there may be focal deficit without a major drop in the level of consciousness. Such penetrations are classified under pTBI and carry the risk of introducing contaminating bacteria into the brain or cerebrospinal fluid.20-22 Our consensus recommendation based on the past guidelines and the recent literature indicates a short-term course of antibiotics, limited superficial debridement, and closure of soft tissues and skin. These patients are followed with contrast enhanced CT scans to look for the very low probability of abscess formation. The case example presented here (left) was a 21-year-old soldier with a right frontal penetrating injury who was fully conscious and complained of some headache and left sided hemiparesis. The one-inch diameter wound was locally debrided, the soft tissues were cleaned with antiseptics, and the wound was closed with monofilament nylon. The patient was kept on broad-spectrum antibiotics for 5 days. He remained infection-free one year after his pTBI and the left sided weakness had improved to a major extent. Case example # 2 was a 12-y-o boy with an air-gun pTBI who was admitted to the trauma center with head ache and no neurological deficit. The pellet penetrated the right temporal tip without intracranial retained bone fragments or hematoma. The entrance wound was locally debrided and closed and the patient was kept on antibiotics for 5 days with antiepileptic medications for 7 days. Six months following pTBI incident the patient remains neurologically intact with no evidence of intracranial infection or post-traumatic seizures.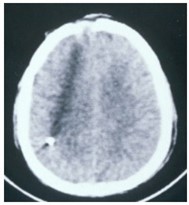 Figure 1
Figure 1 Figure 2
Figure 2 - Expert Opinion
Do all penetrating injuries need radical or conservative tract debridement? The added very low or low level evidence adds to that considered in the 2001 guidelines to support local wound debridement and closure as a viable option for select victims of pTBI. The concept is much more meaningful in mass casualties and when low energy pellets accidentally penetrate skull and non-eloquent brain and cause no deficit. In such circumstances a short term course of antibiotics following local debridement and closure of scalp and re-evaluation of brain tract by contrast CT seems to be an acceptable recommendation.
- Future Directions
Wound management studies in low velocity pTBI patients seem feasible and ethically acceptable. Prospective observational studies at a time when mass casualties harm a large number of patients could shed some light into the risk of deep brain infections or seizures when tract exposure and debridement in an operating room is not performed.