- Futility Assessment Toolkit
In order to fully understand the approach adopted by the current subject matter experts concerning this "Futility Assessment", an understanding of the prior, first edition of these penetrating head injury guidelines is necessary
7 . The following summary addresses the approach previously adopted.Prior (First Edition) Penetrating Head Injury Guidelines
The previously published Guidelines for the Management of Penetrating Brain Injury included a large section devoted to prognostication
7 . This term is generally taken to mean a forecast of the likely course of a disease or ailment. The document presented "early clinical indicators that may be prognostic of outcome among patients with penetrating brain injury (PBI)."While studies referencing outcome stratification based on GOS were included, the primary outcome that was addressed in this section was death. The prognostic indicators selected included those "clinical assessments derived from measures with proven reliability," with reliability defined by the prior authors to mean "that different people with different backgrounds will reach the same conclusion about what they observe most of the time7 ." The prognostic factors included Demographics (Age), Epidemiology (cause of injury, mode of injury, caliber of weapon), Systemic measures (hypotension, coagulation disturbances, respiratory distress), Neurologic measures (Level of Consciousness and GCS score, pupillary examination, intracranial pressure), and neuroimaging features (missile track, evidence of increased intracranial pressure, presence of hemorrhage or mass lesion)7 .From the methodologic perspective, the authors of the prior guidelines determined that recommendations, reserved for therapeutic interventions, were not possible concerning prognosis. Instead, conclusions rather than recommendations were presented. Further, the authors also concluded that articles concerning prognosis, largely observational in nature, could not be evaluated based on the same methodology applied to those pertaining to therapeutic intervention (see reference on prior pTBI guidelines methodology). They therefore derived, based on their expert opinion, five criteria that generally characterized the strongest prognostic studies: 1) Patients should be seen at a uniform time in their disease, 2) Patients should be followed prospectively for a designated block of time, 3) patients should have their outcomes measured definitively and reliably, 4) included patients should be part of a continuous or defined cohort of at least 25 patients, and 5) patients should be examined for extraneous prognostic variables, such as underlying disease or age. Prognosis articles were then classified as class I (all five of the above characteristics), class II (four of the above five characteristics, and class III (three or fewer of the above characteristics.
A total of 24 studies were included as direct evidence for review and analysis
23-45 . The conclusions below from the first edition were reviewed by the panelists of this second edition. We queried our panelists through the blinded Delphi process to determine if expert opinion felt these were still valid and relevant prognosticators. The factors below were ratified by our group as still being relevant and important prognosticators with at least an 80% level of consensus:- Increasing age correlates with increased mortality after penetrating brain injury (Class III)
- Suicide is correlated with a higher rate of mortality than other causes of PBI (Class II)
- Perforating injuries correlate with a poorer outcome when compared with either penetrating or tangential brain injuries (Class III)
- The effect of weapon caliber on outcome, independent of total kinetic energy, was not demonstrated in published data
- Hypotension is associated with increased mortality (class III)
- Coagulopathy is associated with increased mortality, particularly at lower levels of the GCS (Class III)
- Respiratory distress is associated with increased mortality (Class III)
- In civilian patients, low GCS correlates with higher mortality and unfavorable outcome (Class I). In military injuries, fewer patients have a low GCS score. A strong correlation also exists between low GCS score and unfavorable outcome in military series (Class III)
- The presence of bilateral fixed and dilated pupils is highly predictive of mortality (Class III)
- High ICP is predictive of higher mortality (Class II)
- Bi-hemispheric lesions relate to increased mortality (Class II). Compared with uni-lobar injuries, multi-lobar injuries are strongly associated with mortality (Class III). Injuries with ventricular involvement have an increased mortality rate (Class III)
- Cisternal effacement in severe PBI is associated with increased mortality (Class I). No relation between midline shift and outcome has been established (Class I)
- Intraventricular hemorrhage is strongly correlated to increased mortality (Class I). Subarachnoid hemorrhage is also correlated to increased mortality (Class I)
It must be stressed again that the above represent conclusions based on selected literature with a relatively unique methodology developed by the prior subject matter experts that to our knowledge has not been validated. These indicators were considered reliable as defined above. It must also be stressed that the prognosis section of the prior guidelines
7 was a monumental effort, and stood alone as the single largest section of the prior guidelines.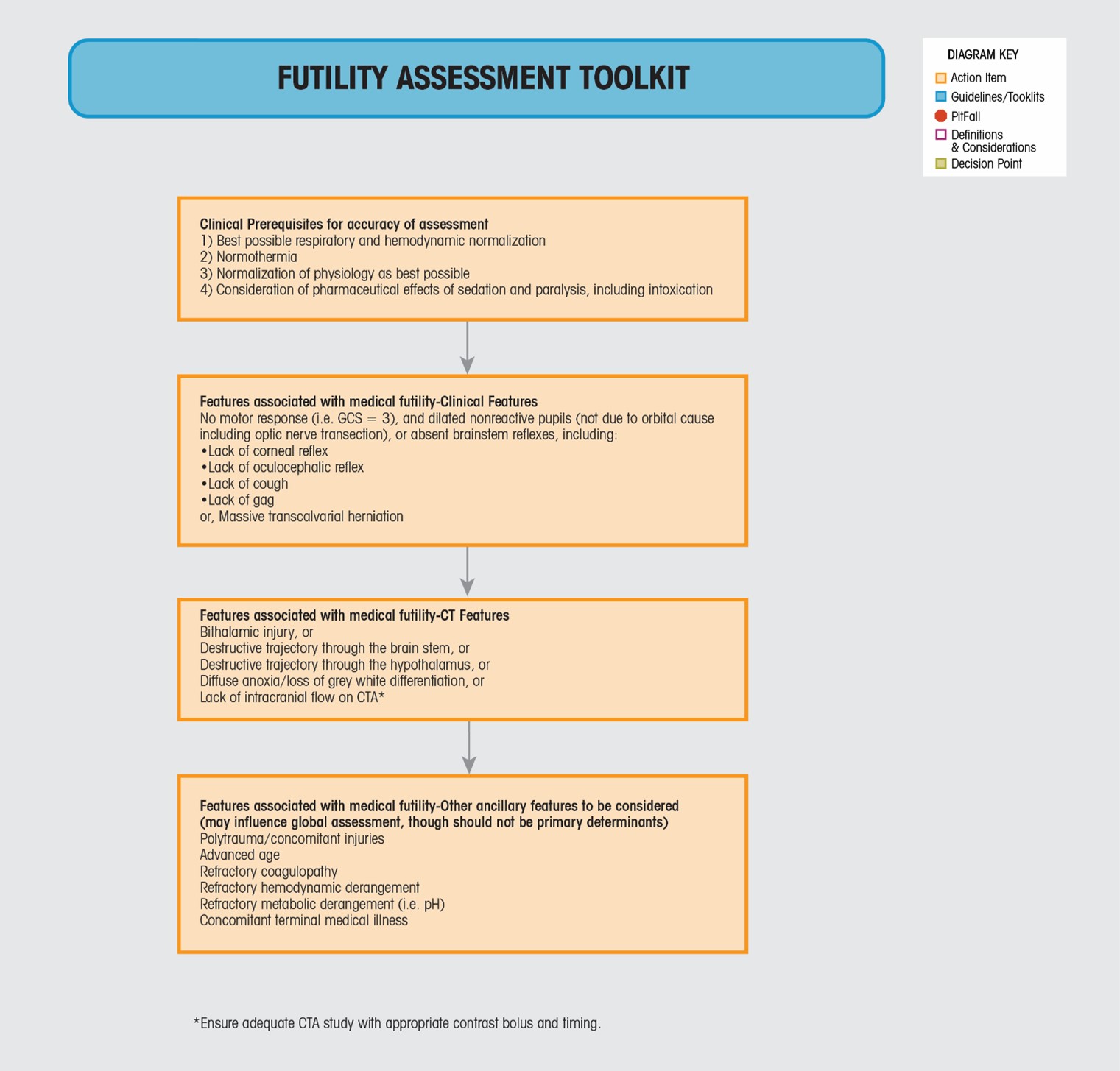
Current Guidelines and Algorithm
There was considerable debate on the topic of Prognosis before and during the BTF pTBI In-Person Guidelines Meeting in September, 2023. The most intense discussion centered around the perceived unintended effect of the inclusion of a section on prognosis in the prior guidelines
7 . Specifically, and after reviewing the above conclusions, the reader is left with multiple clinical indicators associated with mortality and unfavorable outcome, and none associated with survival. This despite the direct statement from the prior authors that "...among survivors, the percentage of patients with favorable outcome is equal [when comparing populations with closed and penetrating brain injury]...Consequently, the main difference in outcome between penetrating and nonpenetrating injury is the difference in mortality." (prior prognosis guidelines, S46)7 . Nevertheless, in a busy, abstract or executive summary focused world, the above statement buried in text was under-emphasized. While the above prognosis recommendations are accepted as valid, and are in fact used as the foundation for current valid prognostic calculators like the SPIN score46,47 , it was the opinion of the current expert group that these prognosis conclusions may have had the unintended effect of biasing the reader toward the nihilistic impression that intervention in pTBI may be futile. Said differently, it was the considered and universal opinion of the authors that decision making based on possible outcomes (death) derived from mostly retrospective literature (prior guidelines) in an area of TBI biased by therapeutic nihilism has potentially resulted in the loss of many lives.Additional discussion centered on the possible purpose of including prognostic factors. The prior authors keenly point out that recommendations could not be made because therapeutic interventions were not being evaluated and proposed
7 . This reinforces the understated fact that the included studies referred to outcomes based on the clinical indicators listed above, without stratification of outcome in the same populations based on any intervention. As we found in our effort, and in sympathy with the prior authors, there is only one study in pTBI that prospectively stratified a pre-specified outcome based on an applied intervention13 . This lead us to conclude that the possible purpose of including a section on prognosis might have been to aid the neurosurgeon or trauma surgeon in clinical decision making by utilizing one or more prognostic variables to determine which patient is likely to benefit from aggressive surgical intervention. This guidance, however, was neither referenced nor included as the stated intent in the prior guidelines. Furthermore, as written, the conclusions would lead the reader to decide early who is likely to die rather than who will benefit from intervention. The current subject matter experts could only conclude that the purpose of including prognostic variables in the prior guidelines effort was simply to provide information on this subject, without specific guidance concerning how the information provided should or may be applied. As previously stated, it was the opinion of the current authors that this had the unintended consequence of biasing neurosurgeons towards non-intervention.With this in mind, it was not disputed that the prior prognosis variables remain valid. The decision was therefore made to review and ratify the prior prognosis variables or not. This ratification was accomplished based on our published methodology, with 80% of those voting necessary to achieve consensus. Each of the above prognosis recommendations was subject to blind voting, with the percent consensus included below. Note, not all prior conclusions were ratified by the current authors.
It was subsequently concluded by our group by formal vote that, while the prior prognosis variables may be valid, initial decisions concerning intervention or non-intervention should be made, not based on the possibility of a particular long-term outcome, but instead based on medical futility of any proposed intervention. As stated above, we accepted the definition of medical futility as "A proposed therapy should not be performed because available data show that it will not improve the patient's condition"
22 . In short, rather than deciding to intervene based on how we think a patient will do in the long-term, we are recommending that decisions to intervene in pTBI be based on whether or not the proposed intervention is predicted to help the patient. The prior prognosis recommendations and observations may then be utilized, after the acute period, to facilitate counseling of the patient's family/surrogate decision maker.Why did we choose this approach? Recent evidence
48,49 indicates that, with few exceptions, we as neurosurgeons do not accurately predict long-term outcomes in traumatic brain injury. Further, in our opinion, non-intervention should be limited to circumstances strongly believed to be associated with futility, with bias towards initial intervention in the interest of preserving life and the opportunity for best possible outcome.With this in mind, the Futility Assessment Toolkit was created. This assessment was the product of many hours of debate, and it ultimately achieved 100% consensus from the authors in its final form. It must be stressed that this assessment is based on expert consensus opinion in the absence of evidence. There is limited evidence base that directly supports what is proposed, and this assessment will require future outcome validation. There are obvious similarities between our proposed Futility Assessment and established processes for brain death testing. This assessment stresses first the clinical prerequisites for accuracy of assessment. These include achieving the best possible respiratory and hemodynamic normalization, normothermia, normalization of general physiology to the best extent possible, and consideration of the pharmaceutical effects of sedation, paralysis, and other intoxicating agents. These recommendations define the post-resuscitation patient status, align directly with ATLS and other guidelines
50,51 . This is critical to ensure with the highest possible certainty that brain function is being accurately assessed in the absence of confounders.The imaging features associated with medical futility include destructive trajectories through the brainstem, bilateral thalamus, or bilateral hypothalamus (zona fatalis), known to be fatal
52 . Additional imaging features include diffuse loss of grey white differentiation, and lack of intracranial flow noted on CTA. From an application perspective, any one of these features may be considered a primary determinant of medical futility. We acknowledge that a lack of intracranial blood flow on a properly performed CTA is generally considered insufficient in the distinct context of a brain death assessment. We have chosen this criteria, however, as a CTA is typically performed early in the course of care before the critical decision to perform or not perform a brain surgery is made and because absent intrancranial flow on a CTA is clearly a poor prognosticator despite being insufficiently rigorous for a brain death assessment. Care should be taken in this specific modality to ensure appropriate contrast administration.The clinical features chosen include no motor response as seen with true GCS=3 (post-resuscitation, non-pharmacologic; see above), bilateral dilated and non-reactive pupils (non-pharmacologic, not associated with orbital injury), absent brainstem reflexes, and massive trans-calvarial brain herniation. From an application perspective, any one of these features may be considered a primary determinant of medical futility.
The final section provides guidance concerning ancillary clinical and demographic features that may be considered. As stated, these may influence global assessment, may aid in counseling clinical and family medical decision makers, but should not be utilized in isolation as primary determinants of medical futility.
In summary, the purpose of the Futility Assessment is to encourage biasing initial, time sensitive, neurosurgical and other clinical decision making in patients with pTBI toward intervention rather than non-intervention, excluding those circumstances where intervention is considered medically futile. The following algorithm slides and discussion pre-suppose that a futility assessment has been performed, and intervention is considered not medically futile.
- Futility Assessment ToolkitFutility Assessment Toolkit
Clinical Prerequisites for accuracy of assessment
- Best possible respiratory and hemodynamic normalization
- Normothermia
- Normalization of physiology as best possible
- Consideration of pharmaceutical effects of sedation and paralysis, including intoxication
Clinical Features associated with medical futility
No motor response (i.e. GCS=3), and dilated nonreactive pupils (not due to orbital cause including optic nerve transection),
or absent brainstem reflexes, including:
- Lack of corneal reflex
- Lack of oculocephalic reflex
- Lack of cough
- Lack of gag
or massive transcalvarial herniation
CT Scan Features associated with medical futility
- Bithalamic injury, or
- Destructive trajectory thru brain stem, or
- Destructive trajectory thru hypothalamus, or
- Diffuse anoxia/loss of grey white differentiation, or
- Lack of intracranial flow on CTA (ensure adequate CTA study with appropriate contrast bolus and timing)
Other/Ancillary Features associated with medical futility
- Polytrauma/concomitant injuries
- Advanced age
- Refractory coagulopathy
- Refractory hemodynamic derangement
- Refractory metabolic derangement (i.e. pH)
- Concomitant terminal medical illness